Open Access | Research
This work is licensed under a Creative Commons Attribution-ShareAlike 4.0 International License.
Sensory reweighting patterns and fall history in early geriatric age: implications for physiotherapy assessment
* Corresponding author: Wittaya Duangnga
Mailing address: Faculty of Physical Therapy, Huachiew Chalermprakiet University 18/18 Thepharat Road, Samut Prakan,
Thailand.
Email: wittaya.dua@hcu.ac.th
Received: 01 March 2026 / Revised: 02 April 2026 / Accepted: 18 April 2026 / Published: 30 June 2026
DOI: 10.31491/APT.2026.06.221
Abstract
Background: Falls are a leading cause of injury and functional decline among older adults. Although fall rates increase with advanced age, early alterations in postural control may already be present in early geriatric age. Postural stability depends on dynamic sensory reweighting among visual, somatosensory, and vestibular inputs. Subtle impairments in this adaptive process may not be detected during routine quiet standing under stable conditions. This study aims to investigate sensory reweighting indices based on center of pressure (CoP) sway area under four standardized sensory conditions and determine their ability to discriminate fall history in early geriatric age.
Methods: This secondary cross-sectional analysis included 34 adults aged 60–70 years (9 fallers, 25 non-fallers). Postural sway was recorded during quiet standing under four conditions: firm surface eyes open (Firm-EO), firm eyes closed (Firm-EC), foam eyes open (Foam-EO), and foam eyes closed (Foam-EC). Three indices were calculated:
visual dependency index (VDI), somatosensory vulnerability index (SVI), and postural adaptability index (PAI). Between-group differences were assessed using the Mann–Whitney U test. Logistic regression and receiver operating characteristic (ROC) analyses were performed to explore associations and discriminative performance.
Results: Fallers demonstrated significantly higher PAI values than non-fallers (P = 0.024), indicating reduced adaptability under escalating sensory challenge. SVI under eyes-closed conditions approached significance (P = 0.055). ROC analysis showed acceptable discrimination for PAI (AUC = 0.756, 95% CI 0.569–0.942, P = 0.007) and SVI_EC (AUC = 0.720, P = 0.011). Logistic regression revealed a positive, though non-significant, association between PAI and fall history (OR = 1.13, P = 0.075).
Conclusion: Early geriatric age with fall history exhibit impaired postural adaptability under multisensory challenge. Sensory-derived adaptability indices may provide additional insight beyond absolute sway magnitude and support early identification of fall vulnerability. However, their role in fall risk identification requires further validation.
Keywords
Balance, early geriatric age, postural sway, center of pressure, fall
Introduction
Falls are a major cause of injury, disability, and healthcare utilization among older adults [1, 2].
While fall incidence increases markedly in advanced age, early alterations in postural control may emerge during the early geriatric
stage (60–70 years) [3, 4]. Identifying early changes in balance control mechanisms is therefore essential for preventive physiotherapy practice [5].
Postural stability relies on the coordinated integration of visual, somatosensory, and vestibular inputs [6–9]. Under stable environmental conditions, redundant sensory information allows efficient maintenance of upright stance [8, 10]. When specific sensory channels are altered, such as during eye closure or standing on a compliant surface, the central nervous system must dynamically adjust the relative contribution of each sensory modality [8, 11]. This adaptive process, commonly termed sensory reweighting, enables maintenance of stability despite changing environmental constraints [6, 8].
Age-related changes in sensory systems, including reduced plantar sensation, diminished proprioceptive acuity,
and visual decline, may influence this adaptive process [5, 6]. Inefficient sensory reweighting may result in excessive reliance on visual input or difficulty adapting to somatosensory perturbations [6, 12, 13]. Importantly, such alterations may not be apparent during routine quiet standing on a firm surface with eyes open, a condition frequently used in clinical settings [5].
Previous studies have reported altered sensory integration in advanced older adults and neurological populations [6]. However, evidence regarding early geriatric age remains limited [11]. Most investigations have emphasized absolute sway magnitude rather than examining how stability changes across progressively challenging sensory contexts [5, 11]. From a physiotherapy perspective, understanding patterns of sensory dependency may provide insight into underlying mechanisms of instability and inform targeted intervention strategies [6, 8].
Center of pressure (CoP) analysis offers an objective method for quantifying postural sway [5, 11, 14]. Measures such as sway area are sensitive to sensory manipulations and have demonstrated utility in identifying individuals at elevated fall risk [15, 16]. Nevertheless, evaluating CoP metrics in isolation may not fully capture how individuals adapt to sensory perturbations [5]. Deriving indices that reflect changes across standardized sensory conditions may provide clinically meaningful information regarding sensory integration strategies [7].
Therefore, this study aimed to examine sensory reweighting patterns derived from CoP sway area across four standardized sensory conditions in early geriatric age and to determine their association with fall history. We hypothesized that individuals with a history of falls would demonstrate increased visual dependency under somatosensory challenge and reduced adaptability across escalating sensory conditions.
Methods
Study design
This study was a secondary analysis of an established balance database [11, 17]. Ethical approval was obtained for the original data collection [11].
Participants
Participants aged 60–70 years were included. Fall status was determined based on self-reported falls within the previous 12 months. Individuals were categorized as fallers (≥ 1 fall) or non-fallers (no falls).
Postural assessment protocol
Postural sway was recorded during quiet standing under four standardized sensory conditions adapted from the sensory organization framework described by Santos and Duarte [11]. This protocol systematically manipulates visual and somatosensory inputs to examine adaptive sensory integration during upright stance. The four conditions were firm surface eyes open (Firm-EO), firm surface eyes closed (Firm-EC), foam surface eyes open (Foam-EO), and foam surface eyes closed (Foam-EC).
CoP sway area was extracted for each condition. To characterize sensory integration patterns beyond absolute sway magnitude, three sensory-derived indices were calculated:
• VDI: ratio of eyes-closed to eyes-open sway within the same surface condition (EC/EO), reflecting reliance on visual input.
• SVI: ratio of foam to firm surface sway (Foam/Firm), reflecting sensitivity to altered somatosensory input.
• PAI: relative change in sway from the least challenging condition (Firm-EO) to the most challenging condition (Foam-EC), representing overall adaptability across escalating sensory demands.
Higher index values indicated greater instability under sensory challenge and were interpreted as reflecting less efficient sensory integration.
Data preprocessing
For each participant, CoP sway area was calculated as the mean of three trials within each of the four standardized sensory conditions. Complete data were available for all participants across conditions; consequently, all 34 subjects were retained for statistical analyses.
Statistical analysis
Between-group differences were assessed using the Mann–Whitney U test. Associations between sensory reweighting indices and fall history were examined using binary logistic regression modelling. Discriminative ability was evaluated through receiver operating characteristic (ROC) curve analysis, with the area under the curve (AUC) reported alongside 95% confidence intervals. Statistical significance was set at P < 0.05.
Descriptive statistics, non-parametric group comparisons, and ROC analyses were performed using IBM SPSS Version 31.0.1.0 (IBM Corp., Armonk, NY, USA). Logistic regression analyses were conducted using MATLAB (MathWorks, Natick, MA, USA).
Results
Participant characteristics
Thirty-four early geriatric individuals (9 fallers, 25 non-fallers) were included in the final analysis. Age did not significantly differ between groups (66.85 ± 2.24 vs. 64.98 ± 2.96 years, P = 0.095). Gender distribution showed a higher proportion of males in the faller group (44.4%) compared with non-fallers (12.0%), although this difference did not reach statistical significance. Participant Characteristics are presented in Table 1.
Table 1.
Participant characteristics.
| Variable | Fallers (n = 9) | Non-fallers (n = 25) | P-value |
|---|---|---|---|
| Age (years) | 66.852 ± 2.239 | 64.983 ± 2.960 | 0.095 |
| Gender | |||
| Male, n (%) | 4 (44.4%) | 3 (12.0%) | 0.061* |
| Female, n (%) | 5 (55.6%) | 22 (88.0%) | |
Note: Fisher’s exact test, *P < 0.05.
Sensory reweighting indices
Group comparisons of sensory-derived indices are presented in Table 2. Fallers demonstrated significantly greater postural adaptability impairment, reflected by higher PAI values (median 13.98 [IQR 8.40]) compared with non-fallers (median 8.52 [IQR 7.05], P = 0.024). SVI_EC showed a near-significant difference (P = 0.055), with fallers exhibiting greater instability under combined somatosensory and visual deprivation. No significant between-group differences were observed for VDI_Firm (P = 0.701), VDI_Foam (P = 0.086), or SVI_EO (P = 0.120).
Table 2.
Sensory reweighting indices in early geriatric age.
| Index | Faller | Non-faller | P-value |
|---|---|---|---|
| VDI_Firm | 1.040 (0.784–1.157) | 0.946 (0.806–1.061) | 0.682 |
| VDI_Foam | 1.373 (1.310–1.644) | 1.253 (1.204–1.334) | 0.082 |
| SVI_EO | 9.835 (8.391–13.127) | 7.874 (5.803–11.403) | 0.114 |
| SVI_EC | 16.020 (11.925–16.692) | 9.911 (6.681–14.963) | 0.053 |
| PAI | 13.980 (12.856–18.068) | 8.520 (7.248–13.904) | 0.024* |
Note: Data expressed as Median (IQR), *P < 0.05 (Mann–Whitney U test). VDI: visual dependency index, SVI: somatosensory vulnerability index, PAI: postural adaptability index.
Discriminative performance
ROC analysis demonstrated that PAI provided moderate discriminative ability for identifying fall history (Table 3 and Figure 1), with an AUC of 0.756 (95% CI 0.569–0.942, P = 0.007). The optimal cut-off value for PAI was 11.500, yielding a sensitivity of 0.778 and specificity of 0.680. Similarly, SVI_EC also showed significant discriminative capacity (AUC = 0.720, 95% CI 0.551–0.889, P = 0.011), with an optimal cut-off value of 10.271, sensitivity of 1.000, and specificity of 0.520. VDI_Foam (AUC = 0.698, P = 0.087, cut-off = 1.306, sensitivity = 0.778, specificity = 0.680) and SVI_EO (AUC = 0.680, P = 0.057, cut-off = 6.982, sensitivity = 1.000, specificity = 0.440) demonstrated moderate but non-significant discrimination. In contrast, VDI_Firm showed limited discriminatory ability (AUC = 0.547, P = 0.699, cut-off = 1.024, sensitivity = 0.556, specificity = 0.680).
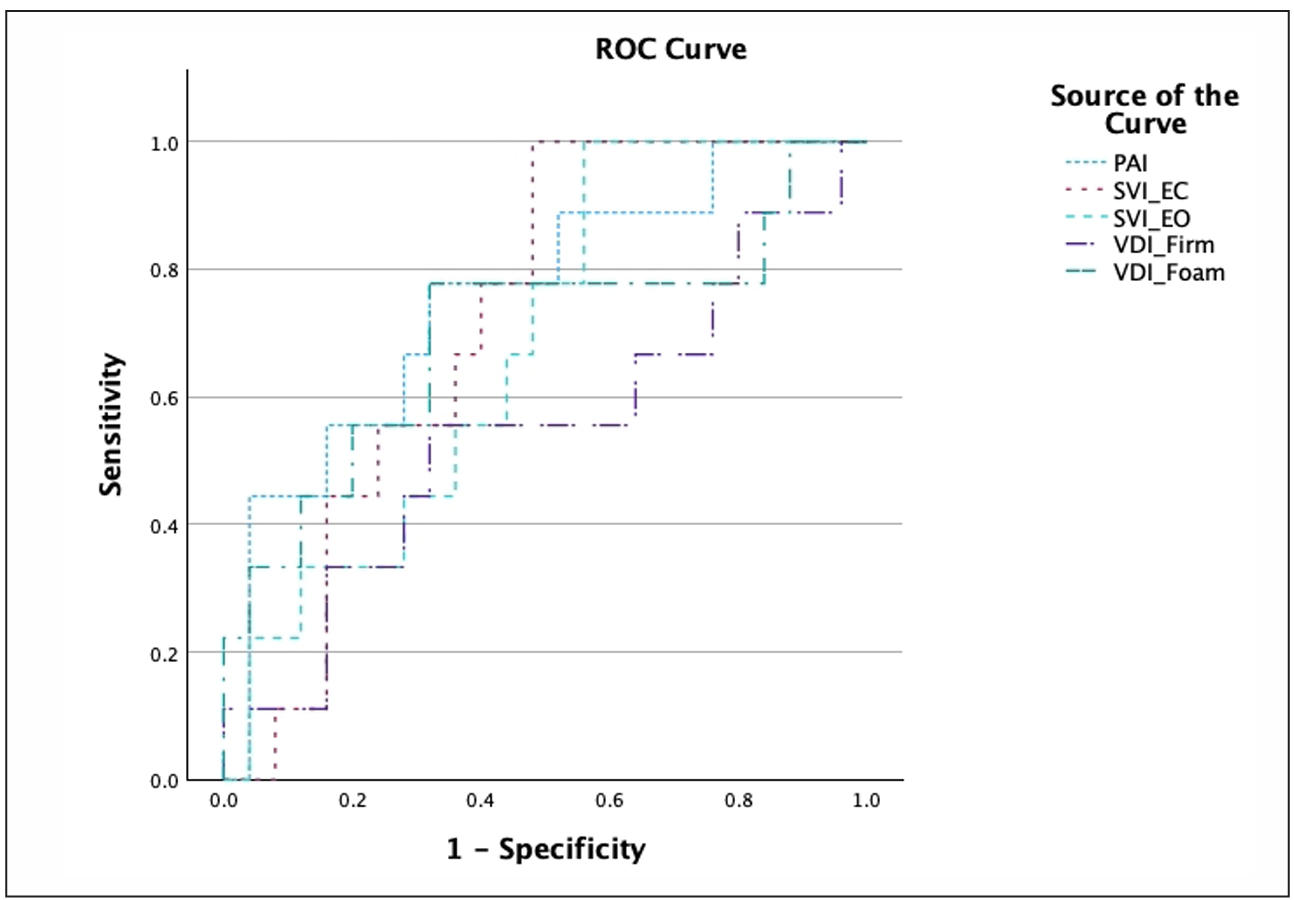
Figure 1. Area under the ROC curve.
Table 3.
ROC analysis of CoP area under sensory conditions.
| Index | AUC | 95% CI | Cut-off | Sensitivity | Specificity | Youden’s index | P-value |
|---|---|---|---|---|---|---|---|
| VDI_Foam | 0.698 | 0.471–0.924 | 1.306 | 0.778 | 0.680 | 0.458 | 0.087 |
| VDI_Firm | 0.547 | 0.310–0.783 | 1.024 | 0.556 | 0.680 | 0.236 | 0.699 |
| SVI_EO | 0.680 | 0.495–0.865 | 6.982 | 1.000 | 0.440 | 0.440 | 0.057 |
| SVI_EC | 0.720 | 0.551–0.889 | 10.271 | 1.000 | 0.520 | 0.520 | 0.011* |
| PAI | 0.756 | 0.569–0.942 | 11.500 | 0.778 | 0.680 | 0.458 | 0.007* |
Note: *P < 0.05, VDI: visual dependency index, SVI: somatosensory vulnerability index, PAI: postural adaptability index.
Logistic regression
Binary logistic regression analysis is presented in Table 4. The results revealed that PAI and SVI_EC were positively associated with fall history. PAI showed a positive association with fall history (OR = 1.124, SE = 0.070, P = 0.075), while SVI_EC also demonstrated a similar trend (OR = 1.120, SE = 0.074, P = 0.106).
Table 4.
Sensory reweighting indices in early geriatric age.
| Predictor | β | SE | OR | P-value |
|---|---|---|---|---|
| SVI_EC | 0.120 | 0.074 | 1.127 | 0.106 |
| PAI | 0.124 | 0.070 | 1.132 | 0.075 |
Note: PAI: postural adaptability index, β: regression coefficient, SE: standard error, OR: odds ratio, *P < 0.05.
Discussions
The present study examined sensory reweighting patterns in early geriatric age and explored their association with fall history. The findings indicate that impairments in postural adaptability, rather than deficits in a single sensory modality, may represent an early indicator of fall vulnerability. Among the evaluated indices, PAI demonstrated the most consistent ability to differentiate fallers from non-fallers, suggesting relatively greater clinical relevance compared with SVI and VDI measures. Importantly, indices derived from single sensory perturbations did not consistently differentiate groups, whereas indices capturing dynamic adaptability across conditions showed stronger discriminatory performance. This pattern highlights the importance of multi-sensory integration processes in maintaining postural stability under progressively challenging conditions.
Sensory reweighting and adaptability
Postural control is not merely the sum of visual, somatosensory, and vestibular inputs, but rather the outcome of continuous sensory reweighting within the central nervous system [8, 14]. Efficient balance requires flexible redistribution of sensory contributions when environmental constraints change [6, 8]. The elevated PAI observed in fallers suggests reduced efficiency in this adaptive process [18]. Importantly, compared with SVI and VDI indices, PAI appears to better capture this dynamic reallocation across progressively challenging conditions,
highlighting its greater sensitivity to early impairments in sensory adaptability.
Rather than exhibiting excessive reliance on vision alone, fallers appeared to demonstrate difficulty when both somatosensory and visual inputs were concurrently degraded [18, 19]. This pattern supports the notion that balance impairment in early geriatric age may emerge under dual-sensory challenge rather than during isolated sensory withdrawal [18]. In contrast, indices derived from single sensory perturbations, such as VDI, may be insufficient to detect these early deficits, as they do not fully reflect the integrative demands placed on the postural control system.
The significant discriminative capacity of SVI_EC may further support this interpretation. When standing on a compliant surface with eyes closed, individuals must rely predominantly on vestibular input and central integration processes [14, 18]. Greater instability in this condition may reflect early inefficiency in sensory integration
mechanisms [12, 18]. However, although SVI_EC demonstrated high sensitivity, its relatively lower specificity suggests a tendency to over-identify individuals as at risk, indicating that it may be more suitable as a screening indicator rather than a standalone diagnostic measure.
Understanding the pattern of sensory reweight allocation in the older adults with a history of falls is important both theoretically and clinically. Clinically, these impaired balance strategies are often not visible during quiet standing on a firm surface with eyes open. This condition is often used in general clinical assessments [18]. Therefore, the assessment that uses brief sensory-challenging conditions may be a highly effective screening tool in the community or clinic setting [18]. Among these, measures reflecting multi-sensory adaptability, such as PAI, may offer greater clinical utility due to their ability to capture cumulative deficits across conditions. In addition, CoP indicators obtained from these conditions can inform the design of physical therapy programs aimed at personalized balance training that targets sensory integration processes before deficits significantly affect function [14, 20]. This approach aligns with early-stage intervention strategies aimed at enhancing adaptive capacity before measurable declines in gross motor function become evident.
Postural adaptability as an early indicator of fall vulnerability
Previous research in advanced older adults and neuro logical populations has reported pronounced sensory integration deficits, frequently characterized by increased visual dependency [8, 18]. In contrast, the present cohort represents an earlier stage of ageing, during which overt instability may not yet be clinically apparent [5,18]. This distinction may explain why indices reflecting single sensory reliance, such as VDI, showed limited discriminative ability in the present study, as early-stage deficits are unlikely to manifest as overt sensory dominance.
The absence of significant differences in indices reflecting isolated sensory withdrawal (e.g., firm surface conditions) suggests that early vulnerability may not arise from dominance of a single sensory modality [18]. Instead, the significant discrimination achieved by PAI and SVI_EC indicates that fall history in early geriatric age may be associated with diminished capacity to adapt under dual-sensory challenge [6, 18]. Notably, PAI demonstrated a more balanced discriminative profile compared with SVI_EC, which showed relatively lower specificity despite high sensitivity, reinforcing the importance of evaluating both detection accuracy and false-positive risk when interpreting these indices. This distinction is clinically meaningful. Visual dependency implies a compensatory strategy, whereas impaired adaptability reflects a limitation in central integration efficiency [8]. The latter may represent a more subtle, preclinical phase of decline, detectable only when the postural control system is sufficiently challenged [18]. Accordingly, assessment protocols incorporating graded sensory perturbations may better capture early balance vulnerability than single-condition testing [5].
Clinical and predictive implications
ROC analysis demonstrated moderate discriminative capacity for PAI (AUC = 0.756) and SVI_EC (AUC = 0.720), indicating limited-to-moderate ability to distinguish between fallers and non-fallers. These findings suggest that indices reflecting multi-sensory adaptability may have potential, but not definitive, clinical utility for fall screening in early geriatric age, which is consistent with previous studies [16]. Given the AUC values observed, these measures should be interpreted as supportive rather than standalone screening tools. Although logistic regression did not reach conventional statistical significance, the direction of the observed associations was consistent with the ROC findings, indicating that greater impairment in adaptability may be related to fall history. However, these associations should be interpreted cautiously due to limited statistical power.
In early ageing populations, event rates are typically lower and functional reserve remains relatively preserved [10, 18]. Consequently, effect sizes may emerge prior to strong statistical prediction. This may partially explain why moderate discriminative performance was observed without statistically significant predictive models. From a physiotherapy perspective, these findings emphasize the value of assessing adaptability under combined sensory challenge [18, 21] and highlight the potential benefit of interventions targeting sensory integration [6] and graded perturbation training [18, 22]. Such approaches may be particularly relevant for early-stage identification and
prevention rather than definitive risk prediction.
Limitations
Several limitations should be considered. First, the cross-sectional design precludes causal inference. Second, the relatively small number of fallers may have resulted in insufficient statistical power. Third, fall history was retrospectively reported and may be subject to recall bias. Fourth, this study constitutes a secondary analysis based on published data, the original study did not provide information regarding the type of falls or the consequences associated with the falls. Fifth, multiple comparisons were conducted without statistical correction, which may increase the risk of Type I error. Therefore, the findings should be interpreted with caution. Finally, although sensory indices provide insight into adaptability patterns, they remain indirect measures of central sensory integration processes. Future longitudinal studies are warranted to determine whether impaired sensory adaptability predicts prospective falls.
Conclusions
This study suggests that early geriatric age with fall history demonstrates reduced postural adaptability under multi-sensory challenge. Indices reflecting dynamic sensory reweighting may provide additional insight beyond traditional sway magnitude measures. However, their role in fall risk identification should be interpreted with caution and requires further validation in larger samples.
Clinical implications
From a physiotherapy perspective, these findings underscore the importance of assessing postural adaptability rather than relying solely on static sway magnitude. Clinical balance assessments that incorporate graded sensory challenges may provide enhanced sensitivity for identifying early fall vulnerability.
Furthermore, rehabilitation programs targeting sensory integration, such as multi-sensory balance training and adaptability-focused interventions, may be beneficial for individuals exhibiting early signs of instability. These approaches may support the maintenance of functional balance capacity rather than serve as definitive fall prevention strategies.
Declarations
Acknowledgments
The author acknowledges the investigators responsible for the Human Balance Evaluation Database (HBEDB) for making the dataset publicly accessible, thereby supporting secondary research in postural control and fall risk assessment. The author also acknowledges institutional supporting us in this research article.
Data availability statement
The data that support the findings of this study are openly available in PhysioNet athttps://doi.org/10.13026/C2WW2W, reference number [11].
Financial support and sponsorship
None.
Conflicts of interest
Not applicable.
Ethical approval and informed consent
This study represents a secondary analysis of de-identified, publicly available data from the Human Balance Evaluation Database (HBEDB). Ethical approval for the original data collection was obtained by the primary investigators [11, 17]. In accordance with local regulations and institutional policies, additional ethical approval was not required for the present analysis of anonymized data.
AI and AI-assisted tools statement
No AI tools were used in the preparation of this article.
References
1. Davis J, Husdal K, Rice J, Loomba S, Falck R, Dimri V, et al. Cost-effectiveness of falls prevention strategies for older adults: protocol for a living systematic review. BMJ Open, 2024, 14: e088536. [Crossref]
2. Montero-Odasso M, Velde N, Martin F, Petrovic M, Tan M, Ryg J, et al. World guidelines for falls prevention and management for older adults: a global initiative. Age Ageing, 2022, 51(9): 1-36. [Crossref]
3. Sukchan P, Prateepko T, Ma-a-lee A, Hounkong K, Sujiwattanarat P, & Piboonpol G. Fall incidences, risk factors, and health effects among early- and middle-aged elderly people in rural areas of border provinces in southern Thailand. J Health Res, 2024, 39(2): 121-134. [Crossref]
4. Joshi R, Tetgure C, & Shah Y. Effect of dual task training versus analogy training on gait speed and balance in older adults—randomized controlled trial. Aging Pathobiol Ther, 2025, 7(1): 56-63. [Crossref]
5. Melzer I, Kurz I, & Oddsson L. A retrospective analysis of balance control parameters in elderly fallers and non-fallers. Clin Biomech, 2010, 25(10): 984-988. [Crossref]
6. Hirata R, Jørgensen T, Rosager S, Arendt-Nielsen L, Bliddal H, Henriksen M, et al. Altered visual and feet proprioceptive feedbacks during quiet standing increase postural sway in patients with severe knee osteoarthritis. PLoS ONE, 2013, 8(8): e71253. [Crossref]
7. Chaikeeree N, Chinsongkram V, & Boonsinsukh R. Interaction of age and foam types used in clinical test for sensory interaction and balance (CTSIB). Gait Posture, 2015, 41: 313-315. [Crossref]
8. Horak F. Postural orientation and equilibrium: what do we need to know about neural control of balance to prevent falls? Age Ageing, 2006, 35: ii7-ii11. [Crossref]
9. Duangnga W, Pannucharoenwong N, Rattanadecho P, Janchomphu W, & Panvichien S. The role of artificial intelligence and machine learning in balance classification using center of pressure-a comprehensive review. Int J Onl Eng, 2026, 22(4): 4–25. [Crossref]
10. Marchetti M, & Whitney S. Postural control in older adults with cognitive dysfunction. Phys Ther Rev, 2006, 11(3): 161-168. [Crossref]
11. Santos D, & Duarte M. A public data set of human balance evaluations. PeerJ Preprints, 2016, 2(4): e2648. [Crossref]
12. Hoorn W, Kerr G, Dieën J, & Hodges P. Center of pressure motion after calf vibration is more random in fallers than non-fallers: prospective study of older individuals. Front Physiol, 2018, 9: 273-285. [Crossref]
13. Laufer Y, Schwarzmann R, Sivan D, & Sprecher E. Postural control of patients with hemiparesis: force plates measurements based on the clinical sensory organization test. Physiother Theory Pract, 2005, 21(3): 163-171. [Crossref]
14. Nakamura J, Nishimae T, Uchisawa H, Okada Y, Shiozaki T, Tanaka H, et al. Effects of postural-control training with different sensory reweightings in a patient with body lateropulsion: a single-subject design study. Physiother Theory Pract, 2024, 40(11): 2701-2711. [Crossref]
15. Kozinc Ž, Löfler S, Hofer C, Carraro U, & Šarabon N. Diagnostic balance tests for assessing risk of falls and distinguishing older adult fallers and non-fallers: a systematic review with meta-analysis. Diagnostics, 2020, 10(9): 667. [Crossref]
16. Oliveira M, Vieira E, Gil A, Fernandes K, Teixeira D, Amorim C, et al. One-legged stance sway of older adults with and without falls. PLoS ONE, 2018, 13(9): e0203887. [Crossref]
17. Goldberger A, Amaral L, Glass L, Hausdorff J, C Ivanov P, Mark R, et al. PhysioBank, physiotoolkit, and physionet: components of a new research resource for complex physiologic signals. Circulation, 2000, 101(23): e215-e220. [Crossref]
18. Shumway-Cook A, & Woollacott M. Motor control: translating research into clinical practice. Wolters Kluwer, Philadelphia, 2017.
19. Peterka R. Sensorimotor integration in human postural control. J Neurophysiol, 2002, 88(3): 1097-1118. [Crossref]
20. Shinohara T, Araki R, Iwamoto H, Igarashi T, Hasegawa S, & Miyata K. Examining the characteristics of balance dysfunction in patients with stroke using item response theory. Physiother Theory Pract, 2025, 41(12): 2549-2559. [Crossref]
21. Boughen J, Nitz J, & Johnston V. Centre of gravity: relevance of behaviour and location in bipedal stance in older adults. Phys Ther Rev, 2017, 22(3-4): 186-196. [Crossref]
22. Maki B, & Mcilroy W. Control of rapid limb movements for balance recovery: age-related changes and implications for fall prevention. Age Ageing, 2006, 35: ii12-ii18. [Crossref]