Open Access | Commentary
This work is licensed under a Creative Commons Attribution-ShareAlike 4.0 International License.
Targeting ageing: the next frontier in drug delivery systems
* Corresponding author: Rajaram Mohapatra
Mailing address: Department of pharmaceutics, School of pharmaceutical science, Siksha 'O' Anusandhan University, Bhubaneswar, Odisha, India.
Email: rajarammohapatra@soa.ac.in
Received: 22 April 2026 / Accepted: 30 April 2026 / Published: 30 June 2026
DOI: 10.31491/APT.2026.06.222
Abstract
Population ageing is rapidly reshaping healthcare systems worldwide, yet most drug delivery systems (DDS) continue to be designed using conventional models that inadequately reflect age-related physiological changes. Ageing is associated with progressive decline in tissue function, altered immune responses, and increased prevalence of chronic diseases, all of which significantly influence therapeutic outcomes. Emerging evidence suggests that biological hallmarks of ageing—including cellular senescence, chronic inflammation, mitochondrial dysfunction, and impaired tissue repair—directly affect drug absorption, distribution, and retention across multiple delivery routes. This commentary discusses how ageing-associated changes compromise the performance of oral, transdermal, ocular, and pulmonary drug delivery systems. Reduced gastrointestinal motility, dysphagia, skin barrier alterations, ocular degeneration, and declining pulmonary function collectively limit the effectiveness of conventional formulations in older adults. Recent advances in sustained-release formulations, biodegradable implants, nanocarriers, and senescence-targeted delivery platforms provide new opportunities to address these challenges. However, elderly populations remain significantly underrepresented in formulation development and clinical translation. We argue that ageing should no longer be treated as a secondary variable in pharmaceutical design. Instead, future DDS development must incorporate age-associated biological mechanisms to create personalized, adaptive, and safer therapeutic strategies for growing elderly populations.
Keywords
Ageing, drug delivery systems, cellular senescence, nanomedicine, elderly therapeutics, precision medicine
Population ageing is rapidly transforming global healthcare priorities. According to the World Health Organization, the number of individuals aged over 60 years is expected to exceed 2.1 billion by 2050, significantly increasing the prevalence of chronic diseases such as cardiovascular disorders, neurodegeneration, diabetes, cancer, and age-related macular degeneration. While therapeutic innovation has advanced considerably, drug delivery systems (DDS) have largely remained “age-neutral,” often overlooking the profound physiological changes that accompany ageing [1, 2]. Recent advances in senescence-targeted therapeutics and precision drug delivery have highlighted an urgent need to redesign
DDS platforms specifically for ageing populations.
A recent wave of studies on senolytics and age-responsive therapeutics has renewed interest in how ageing biology influences drug performance. For example, combinations such as dasatinib and quercetin have demonstrated the ability to selectively eliminate senescent cells in preclinical models, reducing inflammation and improving tissue function [3, 4]. These developments signal an important shift: ageing is no longer viewed solely as a risk factor for disease but as a modifiable biological process that can itself become a therapeutic target. However, the effectiveness of such interventions depends heavily on delivery systems capable of navigating aged tissues [5-7].
Ageing alters nearly every physiological barrier involved in drug transport. In the gastrointestinal tract, reduced gastric acid secretion, delayed gastric emptying, impaired intestinal motility, altered microbiota composition, and reduced transporter activity significantly affect oral drug absorption [8]. Polypharmacy further complicates treatment, as elderly patients frequently require multiple medications with varying pharmacokinetic profiles. Dysphagia also remains a major challenge in older adults, particularly those with neurological disorders, often leading to poor
adherence or unsafe modification of dosage forms [9, 10].
Oral administration remains the most common route of drug delivery, yet ageing significantly alters gastrointestinal physiology. Reduced gastric acid secretion, delayed gastric emptying, altered intestinal motility, microbiome dysbiosis, and reduced transporter expression all contribute to variable drug absorption [10]. Polypharmacy further complicates treatment in older adults. Dysphagia affects a substantial proportion of elderly patients, particularly those with stroke, Parkinson’s disease, and neurodegenerative disorders. Crushing tablets or splitting doses often compromises therapeutic precision. These challenges create opportunities for smarter oral DDS such as gastro-retentive systems, mucoadhesive carriers, multiparticulate formulations, and polymeric microcapsules capable of improving adherence while maintaining controlled release [11].
Transdermal delivery offers several advantages for elderly patients, including improved compliance and avoidance of first-pass metabolism. However, ageing skin undergoes structural deterioration, including epidermal thinning, reduced hydration, decreased lipid content, and impaired dermal blood flow. These changes reduce transdermal permeability and may alter dose consistency. Current patches were not specifically designed for geriatric skin physiology. Future systems may require adaptive adhesives, microneedle-assisted delivery, and stimuli-responsive hydrogels that account for aged skin barriers [12].
Age-related macular degeneration, glaucoma, cataracts, and diabetic retinopathy are increasingly prevalent in ageing populations. Yet ocular drug delivery remains notoriously inefficient. Conventional eye drops deliver less than 2% of administered drug to
intraocular tissues due to tear drainage and poor corneal retention [13]. Age-related reductions in tear production further worsen these limitations. Recent advances in biodegradable implants, nanoparticle carriers, and sustained-release intravitreal systems represent important progress. Anti-vascular endothelial growth factor (anti-VEGF) therapies have demonstrated how delivery innovation can transform treatment outcomes in ageing-related ocular disease [14].
Pulmonary delivery provides rapid systemic absorption and has emerged as an attractive platform for biologics. However, lung ageing introduces new barriers including reduced elasticity, thickened alveolar membranes, impaired mucociliary clearance, and altered immune surveillance. Emerging evidence suggests that age-related changes in pulmonary immune proteins may alter nanoparticle interactions, highlighting the need for immunologically informed inhalation platforms [15]. Figure 1 shows how ageing-associated biological changes impair oral, transdermal, ocular, and pulmonary drug delivery performance and guide advanced therapeutic strategies.
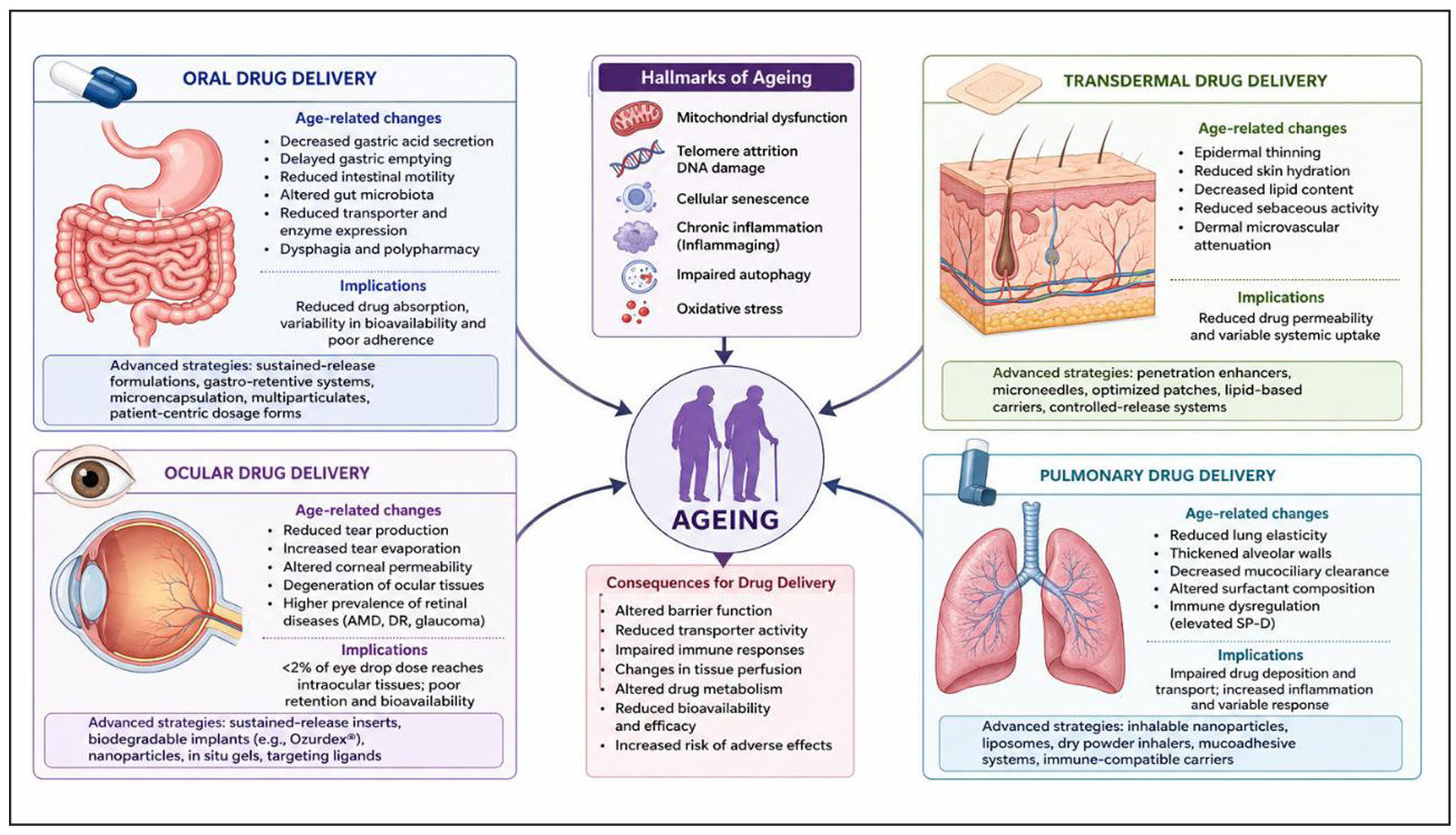
Figure 1. Impact of aging biology on drug delivery performance across major administration routes.
Among all ageing-related mechanisms, cellular senescence may represent the most important future target for DDS innovation. Senescent cells accumulate with age and contribute to chronic inflammation through the senescence-associated secretory phenotype (SASP), which promotes tissue degeneration and disease progression. This has stimulated interest in nanocarriers capable of selectively targeting senescent tissues, delivering senolytic drugs, and minimizing systemic toxicity [16, 17].
Recent developments in biomaterials science are particularly promising. Stimuli-responsive nanoparticles, hydrogel systems, lipid-based carriers, and biodegradable polymeric implants are being engineered
to respond to oxidative stress, inflammatory signals, and pH changes associated with ageing tissues. These systems could enable site-specific drug release while reducing adverse effects associated with conventional formulations [18].
Despite these advances, major challenges remain. Elderly patients are significantly underrepresented in clinical trials evaluating novel DDS platforms. Most formulations are optimized using young animal models or healthy adult populations, limiting translational relevance. Regulatory frameworks also rarely require age-specific delivery evaluation, despite clear physiological differences [16, 19].
Future DDS development must move toward age-adaptive design principles. Rather than treating ageing as a secondary consideration, formulation scientists should incorporate age-associated physiological changes into early-stage drug development. This includes designing dosage forms for patients with dysphagia, creating delivery systems compatible with altered immune function, and engineering carriers that target senescent microenvironments [20].
The future of precision medicine cannot ignore ageing biology. As global populations continue to age, drug delivery technologies must evolve beyond conventional one-size-fits-all approaches. Recent advances in senescence research provide a timely opportunity to rethink how therapeutics are designed, delivered, and optimized for older adults. The next generation of DDS should not simply treat age-related diseases—it should be fundamentally built for ageing itself.
Declarations
Acknowledgements
The authors are grateful to Prof. Monaj Ranjan Nayak, president, Siksha O Anusandhan for his inspiration and facilities.
Availability of data and materials
Not applicable.
Financial support and sponsorship
None.
Conflicts of interests
Not applicable.
Consent for publication
Not applicable.
AI and AI-assisted tools statement
No AI tools were used in the preparation of this article.
References
1. López-Otín C, Blasco M, Partridge L, Serrano M, & Kroemer G. Hallmarks of aging: an expanding universe. Cell, 2023, 186(2): 243-278. [Crossref]
2. Kirkland J, & Tchkonia T. Senolytic drugs: from discovery to translation. J Intern Med, 2020, 288(5): 518-536. [Crossref]
3. Ferrucci L, & Fabbri E. Inflammageing: chronic inflammation in ageing, cardiovascular disease, and frailty. Nat Rev Cardiol, 2018, 15(9): 505-522. [Crossref]
4. Di Micco R, Krizhanovsky V, Baker D, & d’Adda di Fagagna F. Cellular senescence in ageing: from mechanisms to therapeutic opportunities. Nat Rev Mol Cell Biol, 2021, 22(2): 75-95. [Crossref]
5. Sikora E, Bielak-Zmijewska A, & Mosieniak G. Cellular senescence in ageing, age-related disease and longevity. Curr Vasc Pharmacol, 2013, 12(5): 698-706.
6. Mitchell M, Billingsley M, Haley R, Wechsler M, Peppas N, & Langer R. Engineering precision nanoparticles for drug delivery. Nat Rev Drug Discov, 2021, 20(2): 101-124. [Crossref]
7. Anselmo A, & Mitragotri S. Nanoparticles in the clinic: an update. Bioeng Transl Med, 2019, 4(3): e10143. [Crossref]
8. Ezike T, Okpala U, Onoja U, Nwike C, Ezeako E, Okpara O, et al. Advances in drug delivery systems, challenges and future directions. Heliyon, 2023, 9(6): e17488. [Crossref]
9. Chintapula U, Chikate T, Sahoo D, Kieu A, Guerrero Rodriguez I, Nguyen K, et al. Immunomodulation in age-related disorders and nanotechnology interventions. Wiley Interdiscip Rev Nanomed Nanobiotechnol, 2023, 15(1): e1840. [Crossref]
10. Niccoli T, & Partridge L. Ageing as a risk factor for disease. Curr Biol, 2012, 22(17): R741-R752. [Crossref]
11. Elsherbeeny W, El-Gogary R, Nasr M, & Sammour O. Current progress of oral site-specific dosage forms: Emphasis on gastroretentive drug delivery systems. Arch Pharm Sci Ain Shams Univ, 2022, 6(2): 221-238. [Crossref]
12. Alkilani A, Nasereddin J, Hamed R, Nimrawi S, Hussein G, Abo-Zour H, et al. Beneath the skin: a review of current trends and future prospects of transdermal drug delivery systems. Pharmaceutics, 2022, 14(6): 1152-1169. [Crossref]
13. Yadav D, Varma LT, & Yadav K. Drug delivery to posterior segment of the eye: conventional delivery strategies, their barriers, and restrictions. In: Patel J, Sutariya V, Kanwar J, & Pathak Y, editors. Drug Delivery for the Retina and Posterior Segment Disease. Cham: Springer; 2018. p51-67.
14. Tafti M, Fayyaz Z, Aghamollaei H, Jadidi K, & Faghihi S. Drug delivery strategies to improve the treatment of corneal disorders. Heliyon, 2025, 11(2): e41881. [Crossref]
15. Wallin M, Tagami T, Chen L, Yang M, & Chan H. Pulmonary drug delivery to older people. Adv Drug Deliv Rev, 2018, 135: 50-61. [Crossref]
16. Higano N, Thomen R, Quirk J, Huyck H, Hahn A, Fain S, et al. Alveolar airspace size in healthy and diseased infant lungs measured via hyperpolarized 3He gas diffusion magnetic resonance imaging. Neonatology, 2020, 117(6): 704-712. [Crossref]
17. Childs B, Li H, & van Deursen J. Senescent cells: a therapeutic target for cardiovascular disease. J Clin Invest, 2018, 128(4): 1217-1228. [Crossref]
18. Xu M, Pirtskhalava T, Farr J, Weigand B, Palmer A, Weivoda M, et al. Senolytics improve physical function and increase lifespan in old age. Nat Med, 2018, 24(8): 1246-1256. [Crossref]
19. Truong V, Jun M, & Jeong W. Role of resveratrol in regulation of cellular defense systems against oxidative stress. Biofactors, 2018, 44(1): 36-49. [Crossref]
20. Lau S, Schlender J, Slattum P, Heald D, & O'Connor-Semmes R. Geriatrics 2030: developing drugs to care for older persons—a neglected and growing population. Clin Pharmacol Ther, 2020, 107(1): 53-56. [Crossref]