Open Access | Review
This work is licensed under a Creative Commons Attribution-ShareAlike 4.0 International License.
Senotherapeutic potential of Mediterranean diet-derived bioactives in healthy aging and frailty
* Corresponding author: Sedat Arslan
Mailing address: Department of Nutrition and Dietetics, Bursa
Uludag University, Bursa, Turkey.
Email: sedatarslan@uludag.edu.tr
This article belongs to the Special Issue: Effects of Diet and Nutrition on Aging
Received: 02 May 2026 / Revised: 03 June 2026 / Accepted: 09 June 2026 / Published: 30 June 2026
DOI: 10.31491/APT.2026.06.218
Abstract
Population aging is accompanied by an increasing burden of frailty, sarcopenia, metabolic dysfunction, neurodegeneration, and other age-related conditions. Growing evidence suggests that nutrition may influence biological aging through pathways related to cellular senescence, chronic low-grade inflammation, oxidative stress, mitochondrial function, and gut microbiota composition. The Mediterranean diet is one of the most extensively studied dietary patterns for healthy aging and provides a complex matrix of plant foods, extra-virgin olive oil, fiber, unsaturated fatty acids, and diverse bioactive compounds. This review discusses the potential relevance of Mediterranean diet-derived bioactives to senescence-related mechanisms and frailty-related outcomes. Mechanistic links involving inflammatory signaling, redox balance, nutrient-sensing pathways, mitochondrial homeostasis, gut microbiota-mediated immune regulation, and functional decline are considered. Although preclinical evidence supports the biological plausibility of these effects, human evidence remains heterogeneous, and direct clinical proof of senolytic or senomorphic activity from habitual Mediterranean diet exposure is still limited. Therefore, Mediterranean diet-derived bioactives should be interpreted as components of a multi-target nutritional strategy rather than as isolated anti-aging agents. Future studies should integrate dietary assessment, biomarkers of cellular senescence, microbiome and metabolome profiling, inflammatory markers, and standardized functional outcomes to clarify whether Mediterranean diet-based approaches can delay frailty and promote healthy longevity through senescence-related mechanisms.
Keywords
Mediterranean diet, senotherapeutics, healthy aging, inflammaging, frailty
Introduction
Population aging is reshaping the global burden of disease by increasing the prevalence of
frailty, sarcopenia, cognitive decline, cardiometabolic disorders, neurodegenerative
diseases, and multimorbidity. Aging is no longer regarded simply as a chronological
process, but as a complex biological phenomenon characterized by interconnected molecular
and cellular alterations, including genomic instability, epigenetic remodeling,
mitochondrial dysfunction, altered nutrient sensing, chronic inflammation, dysregulated
intercellular communication, stem cell exhaustion, and cellular senescence
[1]. Among these mechanisms, cellular
senescence has gained particular attention because senescent cells can accumulate in
tissues with age and secrete pro-inflammatory, pro-fibrotic, and tissue-remodeling
mediators collectively known as the senescence-associated secretory phenotype (SASP).
This phenotype may contribute to impaired tissue repair, low-grade inflammation,
metabolic dysfunction, and functional decline, thereby linking biological aging with
age-related diseases and geriatric syndromes [1, 2].
Frailty represents one of the most clinically relevant manifestations of biological
aging. It is commonly conceptualized as a state of reduced physiological reserve and
increased vulnerability to stressors, leading to adverse outcomes such as falls,
hospitalization, disability, dependency, and mortality [3].
Although frailty is multifactorial, nutrition is among the most modifiable determinants of its onset
and progression. Inadequate energy and protein intake, micronutrient insufficiency, poor diet quality,
chronic inflammation, oxidative stress, dysbiosis, and reduced muscle anabolism may interact to accelerate physical decline in older adults. Conversely, dietary patterns rich in anti-inflammatory and antioxidant components may support muscle function, immune regulation, metabolic resilience, and healthy aging trajectories [4, 5].
The Mediterranean diet is one of the most extensively investigated dietary patterns in relation to aging and chronic disease prevention. Characterized by high consumption of vegetables, fruits, legumes, whole grains, nuts, olive oil, herbs, and moderate intake of fish and other sources of unsaturated fatty acids, this pattern provides a complex matrix of bioactive compounds, including polyphenols, carotenoids, phytosterols, dietary fiber, monounsaturated fatty acids, omega-3 fatty acids, and micronutrients. Recent evidence suggests that adherence to the Mediterranean diet is associated with lower frailty risk and may contribute to the prevention of sarcopenia and functional decline in older adults [4, 5]. However, the biological plausibility of these effects extends beyond conventional nutrient adequacy. Mediterranean diet-derived bioactives may influence cellular senescence, inflammaging, redox homeostasis, mitochondrial function, gut barrier integrity, and microbiota-derived metabolites, which are increasingly recognized as interconnected mechanisms of healthy aging [6, 7].
The concept of nutritional senotherapeutics has emerged from the broader field of geroscience, in which interventions are evaluated according to their capacity to target fundamental mechanisms of aging rather than single diseases alone. Senotherapeutic strategies are commonly divided into senolytics, which aim to selectively eliminate senescent cells, and senomorphics, which aim to suppress harmful senescence-associated phenotypes without necessarily removing senescent cells [8]. Several plant-derived compounds found in or compatible with Mediterranean dietary patterns, including quercetin, fisetin, resveratrol, oleuropein, hydroxytyrosol, curcumin, and epigallocatechin gallate, have been investigated for their potential to modulate senescence-related pathways in preclinical models [7, 8]. Nevertheless, translating these findings into dietary recommendations requires caution, because the concentrations, formulations, bioavailability, target tissues, and clinical endpoints used in experimental senescence research may differ substantially from habitual dietary exposure in humans.
Therefore, Mediterranean diet-derived bioactives should not be presented as isolated anti-aging agents or substitutes for established clinical care. Rather, they may be better understood as components of a multi-target nutritional strategy that acts through overlapping mechanisms, including attenuation of chronic low-grade inflammation, improvement of oxidative stress responses, modulation of nutrient-sensing pathways, preservation of gut microbiota diversity, and support of muscle and immune function. This review aims to discuss the senotherapeutic potential of Mediterranean diet-derived bioactives in healthy aging, with particular emphasis on their links with inflammaging, gut microbiota, and frailty. By integrating
mechanistic and clinical evidence, this review seeks to clarify both the promise and the current limitations of nutrition-based senotherapeutic approaches for delaying functional decline and promoting healthy longevity.
Methodology
This narrative review was informed by targeted literature searches conducted in PubMed/MEDLINE, Scopus, Web of Science, and Google Scholar from database inception to May 2026. The search strategy combined terms related to the Mediterranean diet and its bioactive components, including "Mediterranean diet," "bioactive compounds," "polyphenols," "olive oil phenolics," "hydroxytyrosol," "oleuropein," "resveratrol," "quercetin," "fisetin," "curcumin," "epigallocatechin gallate," "omega-3 fatty acids, " and "dietary fiber," with terms related to aging biology and geriatric outcomes, including "cellular senescence," "senotherapeutics," "senolytics," "senomorphics," "SASP," "inflammaging," "oxidative stress," "mitochondrial dysfunction," "gut microbiota," "frailty," "sarcopenia," and "healthy aging." Priority was given to mechanistic studies, preclinical evidence, observational studies, human dietary intervention trials, and reviews that directly addressed Mediterranean diet-related bioactives, senescence-related pathways, microbiota-mediated mechanisms, frailty, or sarcopenia. Because the aim was to provide a conceptual and mechanistic synthesis rather than a systematic review, no formal risk-of-bias assessment or meta-analysis was performed. The evidence was interpreted cautiously, with particular attention to distinguishing experimental or supplement-based findings from evidence derived from habitual Mediterranean diet exposure in humans.
Biological aging, cellular senescence, and nutritional senotherapeutics
Cellular senescence is a key mechanism linking biological aging with chronic inflammation,
impaired tissue repair, metabolic dysfunction, and functional decline. Senescent cells are
characterized by stable cell-cycle arrest, resistance to apoptosis, altered metabolic
activity, mitochondrial dysfunction, and secretion of pro-inflammatory and
tissue-remodeling mediators collectively known as the SASP [1, 2].
Although senescence has beneficial roles in tumor suppression, wound healing, and tissue
remodeling, the persistent accumulation of senescent cells during aging may contribute to
inflammaging, impaired regeneration, and age-related clinical phenotypes such as frailty and
sarcopenia [1, 2, 9].
Senotherapeutic interventions are generally classified into two main categories. Senolytics
aim to selectively eliminate senescent cells by targeting their survival pathways, whereas
senomorphics suppress or modify harmful senescence-associated phenotypes, particularly
SASP activity, without necessarily removing senescent cells [8, 10].
A broader and more cautious category may be described as senescence-modulating
interventions, which influence pathways associated with cellular stress, redox balance,
mitochondrial function, nutrient sensing, autophagy, apoptosis resistance, and
inflammatory signaling, but do not provide direct evidence of senescent cell clearance.
This distinction is important when interpreting diet-derived compounds, because most
nutritional exposures are not equivalent to pharmacological senolytic interventions.
Within this framework, the term "nutritional senotherapeutics" should be used cautiously.
Several plant-derived compounds found in or compatible with Mediterranean-style dietary
patterns, including quercetin, fisetin, resveratrol, hydroxytyrosol, oleuropein, curcumin,
and epigallocatechin gallate, have been investigated in relation to senescence-related
pathways [7, 11, 12].
However, much of this evidence comes from cell culture, animal models, or studies using
purified compounds or supplements at doses that may not reflect habitual dietary intake.
Therefore, Mediterranean diet-derived bioactives should not be presented as established
clinical senolytics. A more appropriate interpretation is that they may exert senomorphic,
senolytic-like, or senescence-modulating effects under specific experimental conditions,
while habitual Mediterranean dietary patterns may influence aging biology through cumulative
and indirect mechanisms.
The main pathways through which Mediterranean diet-derived bioactives may intersect
with senescence biology include nuclear factor-κB (NF-κB)-mediated inflammatory
signaling, nuclear factor erythroid 2-related factor 2 (Nrf2)-related antioxidant
responses, AMP-activated protein kinase (AMPK) and sirtuin 1 (SIRT1)-related
nutrient-sensing pathways, mitochondrial quality control, autophagy, gut barrier
integrity, and microbiota-derived short-chain fatty acids (SCFAs). These pathways
are relevant to biological aging, but they are not unique to the Mediterranean diet.
Rather, the distinctive feature of the Mediterranean dietary pattern is that it
combines multiple food-derived bioactives, fiber, unsaturated fatty acids, micronutrients, and nutrient-dense foods
within a whole-diet matrix.
Accordingly, this review uses the term "senotherapeutic potential" as a hypothesis-generating
concept rather than as evidence of proven clinical senolytic activity. The strongest current
interpretation is that Mediterranean diet-derived bioactives may help create a biological
environment less permissive to chronic inflammation, oxidative stress, mitochondrial dysfunction,
dysbiosis, and senescence-associated tissue dysfunction. Whether these effects translate into
measurable reductions in senescent cell burden or clinically meaningful improvements in frailty
trajectories in humans remains an important question for future research.
Mediterranean diet as a multi-target nutritional model for healthy aging
The Mediterranean diet provides a useful model for
healthy aging because it is not defined by a single nutrient, compound, or isolated mechanism. Rather,
it represents a whole-diet pattern characterized by high intake of vegetables, fruits, legumes,
whole grains, nuts, seeds, herbs, and extra-virgin olive oil; moderate intake of fish, seafood,
and fermented dairy products; and relatively low intake of red meat, processed meat, refined grains,
and ultra-processed foods [13, 14].
This dietary structure provides a complex matrix of fiber, unsaturated fatty acids, polyphenols,
carotenoids, phytosterols, vitamins, minerals, and other bioactive compounds that may act through
complementary inflammatory, oxidative, metabolic, vascular, microbial, and immune-related pathways.
From a geroscience perspective, the Mediterranean diet is relevant not because any single
component can be regarded as a proven anti-aging agent, but because the overall dietary
pattern may influence several biological processes that contribute to functional decline.
These processes include chronic low-grade inflammation, redox imbalance, mitochondrial
dysfunction, impaired nutrient sensing, endothelial dysfunction, gut barrier impairment,
dysbiosis, and altered immune-metabolic regulation [1, 6, 13].
These mechanisms are not unique to the Mediterranean diet, and similar pathways may be influenced by
other high-quality dietary patterns. However, the Mediterranean diet is a clinically and
epidemiologically important model because it combines multiple food groups and bioactive
constituents within a pattern that has been extensively studied in relation to cardiometabolic health,
frailty, sarcopenia, and healthy aging [4, 5, 15, 16].
The evidence linking the Mediterranean diet with frailty and functional outcomes is
stronger at the level of dietary patterns than at the level of isolated senotherapeutic
mechanisms. Observational and interventional studies suggest that higher adherence to the
Mediterranean diet may be associated with lower frailty risk, better physical function,
and more favorable aging-related health profiles [4, 5, 16].
The NU-AGE intervention further suggested that a Mediterranean-style dietary intervention may
alter the gut microbiome in older adults in a direction associated with reduced frailty and
improved health status [17]. Nevertheless, these
findings should be interpreted cautiously because Mediterranean diet adherence is also related
to broader lifestyle, socioeconomic, physical activity, and health-related factors, and because
most human studies do not directly measure cellular senescence biomarkers.
Accordingly, the Mediterranean diet should be positioned as a multi-target nutritional model
rather than as a direct senotherapeutic intervention. Its potential relevance to
senescence-related biology lies in the convergence of several indirect and overlapping
pathways: attenuation of inflammaging, improvement of redox balance, support of mitochondrial
and metabolic homeostasis, modulation of gut microbiota-derived metabolites, and preservation
of nutrient adequacy. This framework helps distinguish three levels of evidence: mechanistic
plausibility from cell and animal models, human evidence on Mediterranean diet adherence and
functional outcomes, and the still limited evidence directly linking habitual Mediterranean
diet exposure with validated senescence biomarkers in humans.
This distinction guides the structure of the following sections. Section 4 focuses
on selected Mediterranean diet-derived or Mediterranean-compatible bioactive compounds
and classifies their potential senescence-related actions according to the strength and
type of evidence. Section 5 then synthesizes the major shared pathways, particularly
inflammaging, oxidative stress, and mitochondrial function, while Section 6 focuses
specifically on the gut microbiota as a mediator between Mediterranean diet-derived bioactives
and healthy aging. This organization avoids the interpretation that these mechanisms are
specific to the Mediterranean diet or that they prove direct senolytic activity in humans.
Mediterranean diet-derived bioactive compounds and senescence-related pathways
Mediterranean diet-derived bioactives may intersect with senescence-related biology through inflammatory, oxidative, mitochondrial, metabolic, endothelial, and microbiota-mediated pathways. However, the strength and type of evidence differ substantially across compounds and outcomes. For this reason, it is important to distinguish between three levels of interpretation: experimental evidence from cell culture and animal models, human studies using isolated compounds or supplements, and evidence derived from habitual Mediterranean diet adherence in free-living populations. These levels should not be treated as equivalent (Table 1).
Table 1.
Mediterranean diet-derived bioactive compounds and their potential senescence-related mechanisms.
| Bioactive compound/class | Main Mediterranean dietary sources | Potential senescence-related mechanisms | Relevance to healthy aging and frailty | Evidence level | Proposed senotherapeutic classification |
|---|---|---|---|---|---|
| Hydroxytyrosol and oleuropein | Extra-virgin olive oil, olives, olive leaf-derived products | May modulate oxidative stress, Nrf2 signaling, NF-κB signaling in inflammation, mitochondrial function, proteostasis, and senescence-associated inflammatory signaling | May support vascular, neuromuscular, metabolic, and cognitive resilience by reducing oxidative and inflammatory burden | Strong preclinical and mechanistic evidence; limited direct human senescence biomarker evidence | Hydroxytyrosol and oleuropein: Primarily senomorphic or senescence-modulating; not established senolytic in humans |
| Oleocanthal | Extra-virgin olive oil | May inhibit cyclooxygenase-related inflammatory signaling and modulate inflammatory pathways relevant to chronic low-grade inflammation | May contribute to the anti-inflammatory profile of extra-virgin olive oil and support healthy aging within the whole dietary pattern | Mechanistic and preclinical evidence; limited clinical evidence specific to frailty or senescence | Oleocanthal: Primarily anti-inflammatory/senescence-modulating; not established senolytic |
| Resveratrol | Grapes, berries, peanuts, red wine in moderate cultural contexts | May influence sirtuin 1, AMPK, mitochondrial biogenesis, autophagy, endothelial function, and inflammatory signaling | May support cardiometabolic and vascular health; relevance to frailty is biologically plausible but not established as a dietary anti-aging therapy | Extensive preclinical evidence; heterogeneous human trial evidence | Resveratrol: Senescence-modulating; mainly nutrient-sensing, mitochondrial, and inflammatory pathway modulation |
| Quercetin | Onions, apples, berries, capers, leafy vegetables | May modulate apoptosis resistance, PI3K, NF-κB, oxidative stress responses, and SASP activity | May contribute to reduced inflammatory and oxidative burden; potential relevance to immune-metabolic resilience | Preclinical senotherapeutic evidence; limited human evidence, mostly supplement-based | Quercetin: Senolytic-like in selected preclinical or pharmacological contexts; dietary exposure should be interpreted as senescence-modulating |
| Fisetin | Strawberries, apples, persimmons, grapes, cucumbers | May influence senescent cell survival pathways, apoptosis-related signaling, inflammatory mediators, and oxidative stress responses | Candidate senotherapeutic compound; potential relevance to frailty requires clinical confirmation | Promising preclinical evidence; early and insufficient human evidence | Fisetin: Candidate senolytic in preclinical studies; human dietary relevance remains unproven |
| Curcumin | Turmeric; compatible with Mediterranean-style plant-rich dietary patterns though not a core traditional component | May regulate NF-κB, Nrf2, autophagy, oxidative stress, inflammatory cytokines, and cellular stress responses | May support inflammatory control and metabolic resilience, but clinical relevance depends on bioavailability and formulation | Strong mechanistic evidence; variable clinical evidence | Curcumin: Primarily senomorphic or senescence-modulating; effects depend on dose, formulation, and bioavailability |
| Epigallocatechin gallate | Green tea; compatible with Mediterranean-style dietary patterns though not a core traditional component | May influence oxidative stress, mitochondrial function, inflammatory signaling, autophagy, and metabolic pathways | May contribute to redox and inflammatory balance; direct frailty-related evidence is limited | Mechanistic and preclinical evidence; limited direct geriatric outcome evidence | Epigallocatechin gallate: Primarily senomorphic or senescence-modulating; not established senolytic in humans |
| Carotenoids, including lycopene, lutein, zeaxanthin, and beta-carotene | Tomatoes, leafy greens, peppers, carrots, fruits, herbs | May reduce oxidative damage, support antioxidant defense, modulate immune responses, and protect vascular and visual tissues | May support visual, vascular, cognitive, and immune aspects of healthy aging; indirect relevance to frailty | Moderate observational and mechanistic evidence; limited senescence-specific evidence | Carotenoids, including lycopene, lutein, zeaxanthin, and beta-carotene: Indirect senescence-modulating through redox and immune-related pathways |
| Dietary fiber and microbiota-accessible carbohydrates | Legumes, whole grains, vegetables, fruits, nuts, seeds | May increase SCFAs production, improve gut barrier integrity, modulate immune regulation, reduce endotoxin-related inflammation, and influence histone deacetylase activity | May support gut-immune and gut-muscle axes, reduce inflammaging, and contribute to functional resilience | Strong microbiota-related evidence; emerging evidence for frailty mediation | Dietary fiber and microbiota-accessible carbohydrates: Indirect senescence-modulating through gut microbiota, short-chain fatty acids, barrier function, and immune regulation |
| Long-chain omega-3 fatty acids | Fish and seafood | May promote inflammation resolution, modify cell membrane composition, support mitochondrial function, influence muscle protein metabolism, and reduce catabolic inflammatory signaling | May support muscle function, vascular health, and immune regulation; useful within frailty and sarcopenia prevention strategies | Moderate clinical evidence for inflammatory and muscle-related outcomes; not senolytic | Long-chain omega-3 fatty acids: Indirect senescence-modulating through inflammation resolution, membrane function, and muscle-related pathways; not senolytic |
| Nuts and seed-derived bioactives | Walnuts, almonds, hazelnuts, pistachios, sesame and other seeds | May provide unsaturated fatty acids, vitamin E, magnesium, arginine, phytosterols, polyphenols, and antioxidant compounds that influence endothelial function, oxidative stress, and inflammation | May support cardiometabolic health, satiety, vascular function, and inflammatory balance in older adults | Moderate clinical and observational evidence; limited senescence-specific evidence | Nuts and seed-derived bioactives: Indirect senescence-modulating through cardiometabolic, endothelial, antioxidant, and inflammatory pathways |
| Legume-derived bioactives | Lentils, chickpeas, beans, peas | May provide plant protein, fiber, resistant starch, polyphenols, minerals, and microbial substrates that support short-chain fatty acid production and metabolic regulation | May contribute to protein adequacy, glycemic control, gut health, and functional resilience when tolerated | Moderate evidence for metabolic and microbiota effects; limited direct senescence evidence | Legume-derived bioactives: Indirect senescence-modulating through protein adequacy, fiber fermentation, metabolic regulation, and microbiota-related pathways |
Notes: NF-κB: nuclear factor-κB; Nrf2: nuclear factor erythroid 2-related factor 2; AMPK: AMP-activated protein kinase; SASP: senescence-associated secretory phenotype; SCFAs: short-chain fatty acids; sirtuin 1: SIRT1; phosphoinositide 3-kinase/protein kinase B signaling: PI3K.
In experimental models, several plant-derived compounds found in or compatible with Mediterranean-style dietary patterns have been shown to influence pathways involved in cellular stress responses, apoptosis resistance, SASP activity, mitochondrial quality control, autophagy, and inflammatory signaling [7, 11, 12]. These findings support biological plausibility, but they do not establish that ordinary dietary exposure produces clinically meaningful senolytic effects in humans. Therefore, the compounds discussed in this section are best interpreted as potential senescence-modulating bioactives rather than as established clinical senolytics. The proposed relationships between Mediterranean diet-derived bioactives, shared mechanistic pathways, and frailty-related outcomes are summarized in Figure 1.
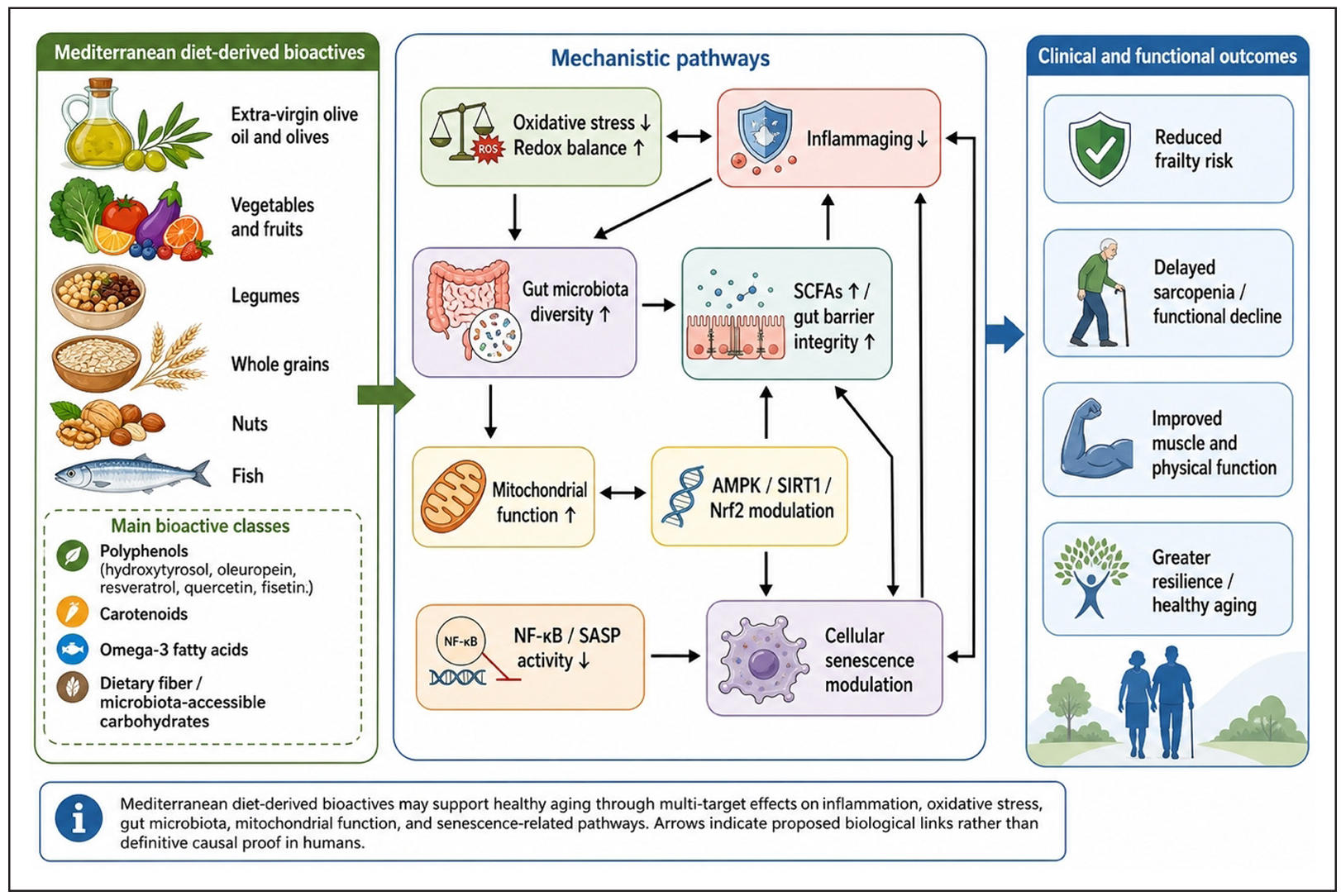
Figure 1. Proposed mechanisms linking Mediterranean diet-derived bioactives with inflammaging, gut microbiota, cellular senescence, and frailty. Mediterranean diet-derived bioactives, including polyphenols, carotenoids, omega-3 fatty acids, and microbiota-accessible carbohydrates, may support healthy aging through multi-target effects on oxidative stress, inflammatory signaling, gut microbiota composition, short-chain fatty acid production, mitochondrial function, nutrient-sensing pathways, and senescence-related mechanisms. These pathways may collectively contribute to reduced frailty risk, delayed sarcopenia and functional decline, improved muscle and physical function, and greater resilience in older adults. Arrows indicate proposed biological relationships rather than definitive causal proof in humans. This figure is an original figure created by the author and was not adapted from a previously published source. AMPK: AMP-activated protein kinase; SIRT1: sirtuin 1; Nrf2: nuclear factor erythroid 2-related factor 2; NF-κB: nuclear factor-κB; SASP: senescence-associated secretory phenotype; SCFAs: short-chain fatty acids.
Extra-virgin olive oil is a defining component of the Mediterranean diet and provides monounsaturated fatty acids together with phenolic compounds
such as hydroxytyrosol, tyrosol, oleuropein, and oleocanthal. Hydroxytyrosol and oleuropein have been investigated for antioxidant, anti-inflammatory, neuroprotective, myoprotective,
and microbiota-related effects relevant to aging [18, 19]. Mechanistically, these compounds may influence redox balance,
inflammatory signaling, mitochondrial function, and proteostasis. However, direct human evidence showing that olive oil phenolics reduce senescent cell burden or
validated senescence biomarkers remains limited. Their relevance is therefore strongest as part of a whole Mediterranean dietary pattern rather than as isolated
senotherapeutic agents.
The compounds listed should be interpreted as potential senescence-modulating dietary bioactives rather than established clinical senolytics. The proposed
senotherapeutic classification is intended to distinguish compounds with direct preclinical senolytic-like evidence from those that may act primarily through
senomorphic, anti-inflammatory, antioxidant, metabolic, mitochondrial, or microbiota-mediated pathways. Evidence levels are qualitative and were assigned according
to the balance of available data as follows: "strong preclinical and mechanistic evidence" indicates repeated support from cell culture, animal, or molecular studies,
but not necessarily direct clinical confirmation; "moderate clinical evidence" indicates the presence of human observational or intervention studies supporting related
inflammatory, metabolic, muscle, microbiota, or functional outcomes, although not necessarily direct senescence endpoints; "limited human evidence" indicates that human
studies are scarce, indirect, supplement-based, heterogeneous, or do not include validated senescence biomarkers; and "senescence-specific evidence" refers only to studies
that directly assess senescence-related markers such as p16INK4a, p21, SASP markers, DNA damage response markers, or related cellular senescence signatures. These
classifications are therefore intended to guide cautious interpretation rather than to provide a formal grading of evidence.
Resveratrol is among the most widely studied dietary polyphenols in aging research. It has been linked to sirtuin 1, AMPK, mitochondrial biogenesis, autophagy, endothelial function, and inflammatory pathways in experimental and
supplement-based studies [20]. Nevertheless,
many reported effects occur at doses or formulations that may not be achievable through ordinary dietary intake. Human trial evidence is heterogeneous and often focuses on
cardiometabolic or inflammatory outcomes rather than direct senescence biomarkers. Thus, resveratrol should be interpreted as a mechanistically relevant compound, but not
as proof that Mediterranean diet exposure has established senolytic activity in humans.
Quercetin and fisetin require particularly careful interpretation because they are frequently discussed in the senolytic literature.
Quercetin is present in onions, apples, berries, capers, and several vegetables, while fisetin is found in strawberries, apples, persimmons,
grapes, and cucumbers. In preclinical and pharmacological contexts, these compounds may influence
senescent cell survival pathways, apoptosis-related signaling, oxidative stress
responses, and senescence-associated inflammatory mediators [11, 12]. However, evidence from purified compounds or
supplement-based protocols cannot be directly extrapolated to habitual dietary intake.
Within a Mediterranean-style diet, quercetin and fisetin are more appropriately described
as contributors to a broader polyphenol-rich pattern with potential senescence-modulating effects.
Curcumin and epigallocatechin gallate are not core traditional Mediterranean diet
components, but they are often discussed in relation to plant-derived compounds with
senescence-modulating potential. Curcumin has been studied for effects on inflammatory
signaling, oxidative stress, autophagy, and cellular stress responses, whereas
epigallocatechin gallate has been linked to redox regulation, mitochondrial function,
inflammatory modulation, and metabolic pathways [7].
Their inclusion in this review should therefore be understood as Mediterranean-compatible or
comparative examples of plant-derived bioactives rather than as defining components of the
traditional Mediterranean dietary pattern. In both cases, clinical translation depends on dose,
formulation, bioavailability, safety, and the use of relevant human endpoints.
Carotenoids, dietary fiber, microbiota-accessible carbohydrates, omega-3 fatty acids, nuts, seeds, and legumes may also contribute to healthy aging, but their
relationship with senescence is largely indirect. Carotenoids may support redox balance,
immune function, vascular health, and visual function [21].
Dietary fiber and microbiota-accessible carbohydrates may promote short-chain fatty acid production,
gut barrier integrity, and immune-metabolic regulation [17].
Long-chain omega-3 fatty acids may support inflammation resolution, membrane function, vascular health,
and muscle-related outcomes [22]. Nuts, seeds, and legumes
provide unsaturated fatty acids, plant protein, minerals, fiber, and polyphenols that may support
cardiometabolic and functional resilience. These components are clinically relevant to aging and
frailty, but they should not be described as direct senolytic interventions.
Overall, Mediterranean diet-derived bioactives provide a biologically plausible framework for linking diet quality with cellular stress responses,
inflammaging, mitochondrial function, gut microbiota, and functional aging. The strongest
evidence currently supports anti-inflammatory, antioxidant, metabolic, microbiota-related,
and functional pathways. The weakest area remains direct evidence that habitual Mediterranean
diet exposure reduces senescent cell burden or improves validated senescence biomarkers in humans.
Future studies should therefore combine detailed dietary assessment with senescence-associated
biomarkers, inflammatory profiles, microbiome data, metabolomics, and functional outcomes such
as grip strength, gait speed, exhaustion, falls, and frailty status.
Inflammaging, oxidative stress, and mitochondrial function
Inflammaging, oxidative stress, and mitochondrial dysfunction are shared biological pathways that may connect diet quality with frailty,
sarcopenia, and functional
decline. These mechanisms are not specific to the Mediterranean diet, nor do they provide direct evidence of senolytic activity. However, they offer a biologically plausible framework for understanding how Mediterranean diet-derived bioactives may support healthier aging
trajectories when consumed as part of a nutrient-dense whole-diet pattern.
Inflammaging refers to chronic low-grade inflammation that develops with aging and may contribute to muscle catabolism, impaired anabolic responses,
fatigue, immune dysregulation, and reduced resilience to stressors [1, 2]. The SASP is one contributor
to this inflammatory environment, but it is not the only source of age-related inflammation. Visceral adiposity, metabolic dysfunction, gut barrier impairment, infections, comorbidities,
and physical inactivity may also contribute. Mediterranean diet-derived polyphenols, unsaturated fatty acids, fiber-rich foods, nuts, legumes, fruits, vegetables, and extra-virgin olive oil may help reduce
inflammatory burden through effects on inflammatory signaling, lipid mediators, gut-derived metabolites, and cardiometabolic health [13, 23, 24]. Nevertheless, most human studies
measure general inflammatory markers rather than direct senescence-related endpoints.
Oxidative stress is another pathway through which Mediterranean diet-derived bioactives may influence aging biology. Excessive or poorly regulated reactive oxygen species can promote lipid, protein, and DNA damage, reinforce inflammatory signaling, impair
mitochondrial function, and contribute to senescence-associated tissue dysfunction [25]. Polyphenols, carotenoids, vitamin E, vitamin C, selenium, zinc,
and other components of plant-rich Mediterranean diets may support redox balance by enhancing endogenous antioxidant defenses, modulating Nrf2-related responses,
reducing oxidative damage, and improving the inflammatory environment [23, 26].
These effects should be interpreted as redox-modulating and cytoprotective rather than as proof of direct senescent cell clearance.
Mitochondrial function is closely linked to muscle performance, energy metabolism, redox signaling, apoptosis, immune activation, and recovery from physiological stress. Age-related mitochondrial dysfunction may contribute to impaired endurance,
reduced muscle strength, metabolic inflexibility, and frailty-related vulnerability [25, 27]. Several Mediterranean diet-derived or Mediterranean-compatible bioactives,
including resveratrol, hydroxytyrosol, oleuropein, quercetin, fisetin, curcumin, epigallocatechin gallate, and omega-3 fatty acids, have been linked in experimental studies to pathways involving SIRT1, AMPK, mitochondrial biogenesis, autophagy, mitophagy,
redox regulation, and inflammation resolution [20, 23, 28, 29]. However, the clinical
relevance of these findings depends on dose, bioavailability, dietary matrix, baseline health status, physical activity, and whether human studies include functional and senescence-related outcomes.
Nutrient-sensing pathways also require careful interpretation in older adults. AMPK, mammalian target of rapamycin, insulin/insulin-like growth factor-1 signaling, and
sirtuins are relevant to autophagy, protein homeostasis, mitochondrial function, and cellular stress responses [1, 28]. Although modulation of these pathways is often discussed as geroprotective,
older adults at risk of frailty or sarcopenia also require adequate energy, protein, micronutrients, and anabolic support. Therefore, Mediterranean diet-based strategies should not prioritize theoretical geroprotective pathway modulation at the expense of muscle preservation, protein
adequacy, and functional capacity.
Overall, the most defensible interpretation is that Mediterranean diet-derived bioactives may attenuate biological conditions that favor senescence-associated tissue dysfunction, including chronic inflammation, redox imbalance, mitochondrial stress, and impaired nutrient sensing. These
effects may contribute to healthier aging and lower frailty risk, but they should be understood as indirect and multi-target actions rather than as demonstrated clinical senolytic effects in humans. Future studies should test this model using integrated endpoints that include inflammatory
markers, oxidative stress indicators, mitochondrial function measures, senescence-associated biomarkers, dietary metabolites, and clinically meaningful outcomes such as grip strength, gait speed, fatigue, falls, hospitalization, disability, and frailty status.
Gut microbiota as a mediator between Mediterranean bioactives and healthy aging
The gut microbiota has become a central component of healthy aging research because it connects diet, immune regulation, metabolism, inflammation, and functional decline.
Aging is often accompanied by reduced microbial diversity, lower abundance of beneficial short-chain fatty acid-producing bacteria, greater inter-individual variability,
increased pathobiont expansion, impaired gut barrier function, and higher susceptibility to inflammation [30, 31].
These changes are not uniform across all older adults, and they are strongly influenced by habitual diet, medication exposure, physical activity, comorbidities, hospitalization,
socioeconomic factors, and living environment. Nevertheless, microbiota-related alterations may contribute to inflammaging, anabolic resistance, immune dysregulation, and frailty progression.
The Mediterranean diet is particularly relevant to the gut microbiota because it provides multiple substrates and modulators for microbial metabolism. Dietary fiber from legumes, vegetables, fruits,
nuts, and whole grains supports microbial fermentation and short-chain fatty acid production. Polyphenols from olive oil, fruits, herbs, nuts, and vegetables can be transformed by gut microbes into smaller
phenolic metabolites with systemic biological activity. Unsaturated fatty acids, plant proteins, micronutrients, and fermented foods may also influence microbial ecology, gut barrier integrity, bile acid metabolism,
and immune signaling [6, 32]. Therefore, the microbiota-related effects of the Mediterranean diet are likely to arise from the
combined influence of food structure, nutrient density, bioactive compounds, and long-term dietary
pattern adherence rather than from any single compound.
The NU-AGE dietary intervention provides one of the most important human datasets connecting Mediterranean diet, gut microbiota, frailty, and healthy aging. In this 1-year intervention across five European countries, adherence to a Mediterranean-style
diet altered the gut microbiome in older adults and was associated with changes linked to reduced frailty and improved health status [17]. The intervention enriched taxa associated with short-chain fatty acid
production and reduced taxa associated with inflammatory profiles. These findings support the idea that diet-induced microbiome modulation may contribute to healthier aging trajectories. However, the study also highlights the complexity of translating
microbiome shifts into clinical recommendations, because individual responses varied and were influenced by baseline microbiota composition, habitual diet, and host characteristics.
Short-chain fatty acids are among the most biologically plausible mediators linking Mediterranean diet adherence with inflammaging and frailty-related outcomes. Acetate, propionate, and butyrate are produced through microbial fermentation of dietary fiber
and resistant starch. These metabolites can influence epithelial barrier integrity, mucin production, regulatory T-cell differentiation, histone deacetylase activity, inflammatory signaling, glucose and lipid metabolism, appetite regulation, and mitochondrial
function [33, 34]. Butyrate is particularly relevant for gut barrier maintenance and anti-inflammatory signaling, while propionate and acetate may contribute to systemic metabolic
regulation. Through these mechanisms, short-chain fatty acids may reduce gut-derived inflammatory stimuli and support immune-metabolic homeostasis in older adults.
Polyphenol–microbiota interactions provide another important link between Mediterranean bioactives and senescence-related biology. Many polyphenols have limited absorption in the upper gastrointestinal tract and reach the colon, where they are metabolized by gut bacteria into
smaller phenolic acids and other metabolites. These microbial transformations may increase or modify biological activity, while polyphenols themselves can shape microbial composition by inhibiting some taxa and supporting others [6, 35].
For example, olive oil phenolics, flavonoids, and other plant-derived compounds may influence microbial metabolites involved in oxidative stress responses, inflammation, endothelial function, and energy metabolism. This bidirectional relationship means that the health effects of Mediterranean polyphenols may partly depend on
the metabolic capacity of an individual’s gut microbiota.
The gut-muscle axis is especially relevant to frailty. Skeletal muscle function is affected not only by protein intake and physical activity but also by systemic inflammation, insulin sensitivity, mitochondrial function, amino acid availability, and microbial metabolites. Dysbiosis may contribute to muscle decline through increased
intestinal permeability, endotoxin-related inflammation, impaired nutrient utilization, and altered bile acid or short-chain fatty acid signaling [36]. Conversely, Mediterranean dietary patterns may support muscle function by combining adequate nutrient density with fiber-driven microbial metabolites, anti-inflammatory bioactives, and cardiometabolic
benefits. Emerging evidence also suggests that specific
gut microbes may be associated with muscle strength,
although causal evidence in humans remains preliminary
and should not yet be translated into probiotic claims.
Gut microbiota may also mediate interactions between Mediterranean diet adherence and cognitive or metabolic aging. Microbial metabolites can influence the gut-brain axis through immune, endocrine, neural, and metabolic pathways, including vagal signaling, tryptophan metabolism, bile acid transformation, and short-chain fatty acid production [37]. These pathways may be relevant to neuroinflammation, blood-brain barrier function, mood, cognition, and neurodegenerative risk. At the same time, the microbiota contributes to cardiometabolic regulation through effects on insulin sensitivity, lipid metabolism, blood pressure, and systemic inflammation. Because frailty frequently coexists with cognitive decline, metabolic dysfunction, and multimorbidity, microbiota-mediated effects may have broad relevance for geriatric health.
Despite this promise, the microbiota should not be presented as a simple causal explanation for the benefits of the Mediterranean diet. Microbiome studies are affected by methodological heterogeneity, including differences in sequencing techniques, taxonomic resolution, statistical analysis, dietary assessment, geographic background, medication exposure, and definitions of frailty. Moreover, microbiota composition is highly individualized, and the same dietary intervention may produce different microbial and clinical responses across older adults. Antibiotics, proton pump inhibitors, metformin, laxatives, polypharmacy, oral health, chewing ability, constipation, and institutionalization may also modify diet-microbiota relationships in aging populations.
Therefore, the most appropriate interpretation is that gut microbiota represents a major mediator and modifier of the relationship between Mediterranean diet-derived bioactives and healthy aging. It may help explain why plant-rich, fiber-rich, polyphenol-rich dietary patterns are associated with lower inflammation and better functional outcomes, but it is unlikely to act independently of broader host and lifestyle factors. Future studies should combine Mediterranean diet interventions with metagenomics, metabolomics, inflammatory biomarkers, intestinal permeability markers, senescence-associated biomarkers, and standardized frailty outcomes. Such integrated designs are needed to clarify whether microbiota-targeted nutritional strategies can meaningfully delay
frailty progression and improve resilience in older adults.
Frailty, sarcopenia, and functional decline
Frailty and sarcopenia are closely related but distinct age-associated conditions that reflect reduced physiological reserve and impaired functional capacity. Frailty is generally characterized by increased vulnerability to stressors, while sarcopenia is defined by progressive loss of skeletal muscle strength, muscle mass, and physical performance
[3, 38]. These conditions frequently overlap in older adults and share several biological drivers, including chronic inflammation, oxidative stress, mitochondrial dysfunction, anabolic resistance, malnutrition, physical inactivity, hormonal changes, multimorbidity, and gut microbiota alterations. Because frailty and sarcopenia are associated with falls, disability, hospitalization, institutionalization, and mortality, they represent clinically meaningful endpoints for evaluating nutritional strategies in healthy aging.
Nutrition is central to the prevention and management of frailty because older adults are vulnerable to both undernutrition and poor diet quality. Reduced appetite, chewing and swallowing difficulties, sensory changes, social isolation, depression, polypharmacy, gastrointestinal disorders, financial constraints, and chronic diseases may reduce energy and nutrient intake. Inadequate protein intake is particularly important because older skeletal muscle shows anabolic resistance, meaning that a higher or more strategically distributed protein intake may be required to stimulate muscle protein synthesis compared with younger adults [39, 40]. European Society for Clinical Nutrition and Metabolism (ESPEN)
guidance emphasizes that older adults should receive adequate energy, protein, micronutrients, and fluid to maintain or improve nutritional status, with higher protein needs in those who are malnourished, at risk of malnutrition, or affected by acute or chronic disease [39].
The Mediterranean diet may contribute to frailty prevention through several complementary pathways. First, it provides high-quality dietary patterns rich in vegetables, fruits, legumes, whole grains, nuts, fish, olive oil, and other nutrient-dense foods. Second, it supplies anti-inflammatory and antioxidant bioactive compounds that may reduce the biological burden of inflammaging. Third, it supports gut microbiota diversity and short-chain fatty acid production through fiber-rich plant foods. Fourth, it may improve cardiometabolic and vascular health, thereby preserving mobility, endurance, and tissue perfusion. Recent review evidence suggests that higher adherence to the Mediterranean diet may delay sarcopenia onset and improve muscle-related outcomes in older adults, although the strength of evidence varies by study design, population, and outcome definition [5].
Frailty is not simply a consequence of low muscle mass; it reflects multi-system dysregulation. The inflammatory phenotype of frailty often includes elevated C-reactive protein, interleukin-6, tumor necrosis factor-α, and other mediators that may impair muscle protein synthesis, increase proteolysis, reduce appetite, alter endocrine signaling, and contribute to fatigue [41]. Oxidative stress and mitochondrial dysfunction may further reduce muscle endurance and repair capacity. Mediterranean diet-derived polyphenols, carotenoids, omega-3 fatty acids, and micronutrients may theoretically reduce these stressors, but their clinical effect depends on the total dietary pattern, baseline nutritional status, physical activity, comorbidities, and adherence. Therefore, a Mediterranean-style diet should be framed as a supportive nutritional pattern for functional resilience rather than as a direct treatment for frailty.
Sarcopenia provides a particularly important bridge between Mediterranean dietary patterns and functional aging. Skeletal muscle is metabolically active and responsive to protein intake, resistance exercise, inflammatory status, insulin sensitivity, mitochondrial function, and hormonal regulation. Mediterranean diets are often discussed for their anti-inflammatory and cardiometabolic benefits, but for sarcopenia prevention, they must also be evaluated for protein adequacy and meal distribution. A plant-forward Mediterranean diet may be nutritionally excellent but still insufficient for muscle preservation if total energy intake, protein quantity, indispensable amino acid content, vitamin D, calcium, and physical activity are inadequate. For this reason, Mediterranean diet-based recommendations for older adults should include practical attention to protein-rich foods such as fish, eggs, dairy products, legumes, and, where appropriate, lean poultry, alongside resistance or multicomponent exercise.
The gut-muscle axis may also help explain the relationship between Mediterranean diet adherence and functional outcomes. Microbial metabolites such as short-chain fatty acids can influence inflammation, insulin sensitivity, mitochondrial function, and immune regulation, all of which may affect muscle performance. Dysbiosis, reduced microbial diversity, and increased intestinal permeability may contribute to systemic inflammation and anabolic resistance in older adults [36]. Mediterranean dietary patterns may counter some of these processes by increasing fiber intake, improving microbiota-accessible carbohydrate availability, and providing polyphenols that are metabolized by gut bacteria into bioactive compounds. However, causality remains difficult to establish because physical activity, medication use, comorbidities, and baseline diet also shape the microbiome and muscle health.
The relationship between Mediterranean diet-derived bioactives and frailty should therefore be interpreted through a systems biology framework. Bioactive compounds may influence cellular senescence, inflammaging, oxidative stress, mitochondrial function, and gut microbiota, while the overall dietary pattern may support nutrient adequacy and cardiometabolic health. These effects may converge on clinically observable outcomes such as grip strength, gait speed, exhaustion, unintentional weight loss, physical activity, falls, and disability. Nevertheless, current evidence is stronger for associations between Mediterranean diet adherence and frailty-related outcomes than for direct proof that Mediterranean bioactives reduce senescent cell burden in humans.
Several methodological limitations must be addressed in future research. Frailty definitions vary widely across studies, including phenotype-based, deficit accumulation, and multidimensional models. Sarcopenia definitions also differ according to criteria, cut-off points, muscle mass measurement techniques, and performance tests. Dietary adherence scores may not capture specific bioactive compound intake, food processing level, protein distribution, or long-term dietary changes. In addition, few studies integrate frailty outcomes with biomarkers of senescence, microbiome composition, inflammatory profiles, and objective physical function measures. These gaps limit the ability to determine whether Mediterranean diet-derived
bioactives act through senescence-related mechanisms or
through broader nutritional and lifestyle pathways.
In clinical practice, the most defensible approach is to use the Mediterranean diet as a flexible dietary pattern that can be adapted to the needs of older adults at risk of frailty or sarcopenia. This means preserving the core features of the diet while ensuring adequate energy, protein, vitamin D, calcium, hydration, and meal feasibility. For older adults with poor appetite, chronic obstructive pulmonary disease, cancer, heart failure, cognitive impairment, or multimorbidity, strict plant-forward recommendations may need to be modified to avoid unintended weight loss or inadequate protein intake. Thus, Mediterranean diet-based strategies for frailty prevention should be individualized, function-oriented, and combined with resistance exercise, fall prevention, social support, and management of underlying disease.
Overall, frailty and sarcopenia are the clinical outcomes that make the senotherapeutic potential of Mediterranean diet-derived bioactives meaningful for geriatric nutrition. The biological rationale is strong: Mediterranean dietary patterns may reduce inflammatory and oxidative stress, support mitochondrial and microbial homeostasis, and provide nutrient-dense foods that preserve physical function. However, the evidence remains insufficient to claim that these effects are mediated primarily by senolytic mechanisms. Future trials should evaluate Mediterranean diet interventions using standardized frailty and sarcopenia criteria, dietary biomarkers, senescence-associated markers, microbiome profiles, and functional outcomes over sufficiently long follow-up periods.
Clinical implications and limitations of the evidence
The clinical relevance of Mediterranean diet-derived bioactives should be interpreted within the broader framework of evidence-based geriatric nutrition. Their main practical value is not as isolated senotherapeutic agents, but as components of a nutrient-dense dietary pattern that may support inflammatory balance, redox homeostasis, cardiometabolic health, gut microbiota composition, and functional resilience. Therefore, clinical translation should focus on the Mediterranean diet as a flexible whole-diet model rather than on high-dose supplementation with individual compounds.
For generally healthy older adults, the Mediterranean diet may be recommended as a preventive dietary pattern that supports overall diet quality and healthy aging. In this group, the emphasis should be on regular intake of vegetables, fruits, legumes, whole grains, nuts, seeds, extra-virgin olive oil, fish, and other nutrient-dense foods, while reducing excessive intake of red meat, processed meat, refined grains, and ultra-processed foods. The potential benefit of this approach is likely to arise from the cumulative effects of fiber, unsaturated fatty acids, polyphenols, carotenoids, micronutrients, and microbial substrates rather than from a single bioactive compound.
For older adults at risk of frailty, Mediterranean diet-based strategies should be more function-oriented. In addition to improving diet quality, clinical attention should be given to adequate energy intake, sufficient protein, vitamin D, calcium, hydration, appetite, chewing ability, meal accessibility, physical activity, and resistance or multicomponent exercise [39]. A plant-rich Mediterranean dietary pattern may support lower inflammatory and oxidative burden, but it should not unintentionally reduce energy intake or protein adequacy in individuals with reduced appetite, unintentional weight loss, or functional decline.
For older adults with malnutrition, sarcopenia, chronic disease burden, or polypharmacy, Mediterranean diet recommendations require further individualization. In these individuals, strict plant-forward advice may need to be adapted to prevent inadequate protein intake, poor energy density, or excessive dietary restriction. Practical strategies may include combining vegetables, fruits, legumes, whole grains, nuts, and olive oil with adequate protein sources such as fish, dairy products, eggs, legumes, and, where appropriate, lean poultry. Nutritional care should also consider medication–nutrient interactions, anticoagulant use, kidney or liver disease, cancer treatment, gastrointestinal tolerance, oral health, and the feasibility of meal preparation.
A clear distinction should also be made between Mediterranean-style foods and concentrated bioactive supplements. Compounds such as resveratrol, quercetin, fisetin, hydroxytyrosol, oleuropein, curcumin, and epigallocatechin gallate may be useful in mechanistic or supplement-based research, but this does not justify presenting them as established anti-aging therapies for older adults. For example, early human senolytic research using pharmacological dasatinib plus quercetin protocols has provided preliminary clinical evidence in disease-specific contexts, but such findings should not be directly extrapolated to habitual Mediterranean dietary exposure or food-based bioactive intake [42].
The evidence base has several limitations. Much of the literature linking Mediterranean diet adherence with frailty and healthy aging is observational, making residual confounding difficult to exclude. Individuals with higher adherence may also differ in physical activity, socioeconomic status, health literacy, smoking exposure, medication use, and access to health care. Intervention trials provide stronger evidence, but many focus on cardiometabolic or inflammatory outcomes rather than frailty, sarcopenia, physical function, or cellular senescence biomarkers. In addition, dietary adherence scores may not capture bioactive compound intake, extra-virgin olive oil quality, food processing level, cooking methods, meal timing, protein distribution, or long-term adherence.
Another important limitation is the lack of direct senescence-related endpoints in most human nutrition studies. Many studies measure inflammatory markers, oxidative stress indicators, metabolic variables, microbiota profiles, or physical function, but these are not specific markers of cellular senescence. Biomarkers such as p16INK4a, p21, senescence-associated β-galactosidase, SASP proteins, DNA damage response markers, and circulating
senescence-related signatures are increasingly discussed in aging research, but they are not yet routinely integrated into dietary intervention trials [43, 44]. Without such markers, it remains difficult to determine whether Mediterranean diet-derived bioactives influence frailty through senescence modulation or through broader anti-inflammatory, metabolic, vascular, microbial, and nutritional pathways.
Overall, the most defensible clinical position is that Mediterranean diet-derived bioactives may contribute to healthy aging as part of a multi-component lifestyle strategy that includes adequate nutrition, resistance exercise, chronic disease management, sleep, social support, and reduction of sedentary behavior. The language of nutritional senotherapeutics should remain cautious and hypothesis-generating until randomized human studies demonstrate that Mediterranean diet-based interventions can modify validated senescence biomarkers and translate these changes into clinically meaningful improvements in frailty, sarcopenia, disability, or quality of life.
Future directions
Future research on Mediterranean diet-derived bioactives and healthy aging should move from broad associations toward mechanism-informed, clinically meaningful, and methodologically integrated study designs. The current evidence supports biological plausibility, particularly through anti-inflammatory, antioxidant, mitochondrial, metabolic, and microbiota-mediated pathways. However, the field still requires human studies that can determine whether Mediterranean dietary patterns or their bioactive components modify senescence-associated biology and whether such changes translate into improvements in frailty, sarcopenia, disability, or other age-related outcomes.
First, future studies should incorporate validated panels of cellular senescence biomarkers rather than relying only on general inflammatory or oxidative stress markers. Potential indicators may include p16INK4a, p21, senescence-associated β-galactosidase activity, DNA damage response markers, SASP proteins, circulating extracellular vesicles, and transcriptomic or proteomic signatures of senescence [43, 45]. Because no single biomarker is sufficient to define senescence in humans, these markers should be interpreted together with clinical and functional outcomes.
Second, clinical endpoints should be standardized and function-oriented. Frailty and sarcopenia are highly relevant outcomes, but their definitions vary across studies. Future trials should use validated frailty tools and consensus-based sarcopenia criteria, together with objective measures such as grip strength, gait speed, chair-rise performance, short physical performance battery, appendicular lean mass, falls, hospitalization, disability, and quality of life [3, 38]. This would help determine whether changes in biological aging pathways are clinically meaningful.
Third, dietary exposure should be measured with greater precision. Mediterranean diet adherence scores are useful, but they may not capture bioactive compound exposure, extra-virgin olive oil quality, food processing level, cooking methods, meal timing, protein distribution, or
long-term adherence. Future studies should combine dietary assessment with biomarkers of intake, such as plasma carotenoids, fatty acid profiles, urinary polyphenol metabolites, and metabolomic signatures of Mediterranean diet adherence [46]. This would reduce measurement error and clarify which components of the dietary pattern are most strongly linked with senescence-related and frailty-related outcomes.
Fourth, microbiome and metabolome profiling should be integrated into clinical nutrition trials. The gut microbiota may mediate or modify the effects of Mediterranean diet-derived fiber, polyphenols, unsaturated fatty acids, and fermented foods. Future studies should include metagenomics, microbial functional profiling, short-chain fatty acid measurement, bile acid profiles, tryptophan metabolites, intestinal permeability markers, and inflammatory mediators [17]. These data would help clarify whether microbiota changes are causal mediators, correlates, or consequences of improved diet quality and health status.
Finally, future trials should be longer, pragmatic, and clinically adaptable. Aging and frailty develop over years, whereas many dietary interventions last only weeks or months. Longer trials with realistic dietary counseling, adherence support, culturally adaptable Mediterranean diet models, and stratified analyses according to age, sex, baseline nutritional status, body composition, frailty risk, sarcopenia, chronic disease burden, medication use, and physical activity are needed. Such studies should also distinguish food-based Mediterranean diet interventions from supplement-based senotherapeutic approaches, because these strategies answer different research questions and should not be interpreted interchangeably.
Conclusions
Mediterranean diet-derived bioactives provide a biologically plausible framework for connecting nutrition with healthy aging and geroscience. As part of a whole-diet pattern, polyphenols, unsaturated fatty acids, dietary fiber, carotenoids, micronutrients, and microbiota-accessible substrates may support healthy aging through multi-target anti-inflammatory, antioxidant, microbiota-related, metabolic, mitochondrial, and possibly senescence-modulating mechanisms. These effects may be relevant to frailty and sarcopenia because they intersect with pathways involved in inflammatory burden, redox balance, gut-immune regulation, muscle function, cardiometabolic health, and functional resilience.
However, Mediterranean diet-derived bioactives should not be interpreted as established clinical senolytics in humans. Current evidence is strongest for mechanistic plausibility and broader diet-related benefits, whereas direct clinical evidence showing that habitual Mediterranean diet exposure reduces senescent cell burden or modifies validated senescence biomarkers remains limited. Therefore, the concept of nutritional senotherapeutic potential should remain cautious and hypothesis-generating. Future studies integrating dietary assessment, bioactive compound biomarkers, senescence-associated markers, microbiome and
metabolome profiling, and standardized frailty and sarcopenia outcomes are needed to determine whether Mediterranean diet-based interventions can meaningfully delay functional decline and promote healthy longevity through senescence-related mechanisms.
Declarations
Author contributions
The author contributed solely to the article.
Availability of data and materials
Not applicable.
Financial support and sponsorship
None.
Conflicts of interest
All author declared that there are no conflicts of interest.
Ethical approval and informed consent
Not applicable.
Consent for publication
Not applicable.
AI and AI-assisted tools statement
During the preparation of this work, the author used ChatGPT, an AI-assisted language tool developed by OpenAI, to support language editing, improve readability, and refine wording. AI-assisted tools were also used to help design and refine the original figure included in the manuscript. After using these tools, the author reviewed and edited all content as needed and takes full responsibility for the content of the published article.
References
1. López-Otín C, Blasco M, Partridge L, Serrano M, & Kroemer G. Hallmarks of aging: an expanding universe. Cell, 2023, 186(2): 243-278. [Crossref]
2. Franceschi C, Garagnani P, Parini P, Giuliani C, & Santoro A. Inflammaging: a new immune-metabolic viewpoint for age-related diseases. Nat Rev Endocrinol, 2018, 14(10): 576-590. [Crossref]
3. Fried L, Tangen C, Walston J, Newman A, Hirsch C, Gottdiener J, et al. Frailty in older adults: evidence for a phenotype. J Gerontol A Biol Sci Med Sci, 2001, 56(3): M146-M156. [Crossref]
4. Gross D, Dahringer J, Bramblett P, Sun C, Spangler H, Lynch D, et al. The relationship between a Mediterranean diet and frailty in older adults: NHANES 2007–2017. Nutrients, 2025, 17(2): 326-339. [Crossref]
5. Arroyo-Huidobro M, Amat M, Capdevila-Reniu A, Chavez A, Pellicé M, Ladino A, et al. The role of the Mediterranean diet in the prevention of sarcopenia and frailty in older adults: a narrative review. Nutrients, 2025, 17(10): 1743-1758. [Crossref]
6. Ticinesi A, Nouvenne A, Cerundolo N, Parise A, Mena P, & Meschi T. The interaction between Mediterranean diet and intestinal microbiome: relevance for preventive strategies against frailty in older individuals. Aging Clin Exp Res, 2024, 36(1): 58-74. [Crossref]
7. Centonze M, Aloisio Caruso E, De Nunzio V, Cofano M, Saponara I, Pinto G, et al. The antiaging potential of dietary plant-based polyphenols: a review on their role in cellular senescence modulation. Nutrients, 2025, 17(10): 1716-1730. [Crossref]
8. Luís C, Maduro A, Pereira P, Mendes J, Soares R, & Ramalho R. Nutritional senolytics and senomorphics: implications to immune cells metabolism and aging—from theory to practice. Front Nutr, 2022, 9: 958563. [Crossref]
9. Gorgoulis V, Adams P, Alimonti A, Bennett D, Bischof O, Bishop C, et al. Cellular senescence: defining a path forward. Cell, 2019, 179(4): 813-827. [Crossref]
10. Saliev T, & Singh P. Targeting senescence: a review of senolytics and senomorphics in anti-aging interventions. Biomolecules, 2025, 15(6): 860-878. [Crossref]
11. Zhu Y, Tchkonia T, Pirtskhalava T, Gower AC, Ding H, Giorgadze N, et al. The Achilles’ heel of senescent cells: from transcriptome to senolytic drugs. Aging Cell, 2015, 14(4): 644-658. [Crossref]
12. Braučič Mitrovic L, & Semen K. Exploring the senotherapeutic potential of polyphenols in aging and disease: a literature review. Int J Mol Sci, 2026, 27(8): 3651-3662. [Crossref]
13. Sofi F, Macchi C, Abbate R, Gensini G, & Casini A. Mediterranean diet and health status: an updated meta-analysis and a proposal for a literature-based adherence score. Public Health Nutr, 2014, 17(12): 2769-2782. [Crossref]
14. Widmer R, Flammer A, Lerman L, & Lerman A. The Mediterranean diet, its components, and cardiovascular disease. Am J Med, 2015, 128(3): 229-238. [Crossref]
15. Casas R, Sacanella E, Urpí-Sardà M, Chiva-Blanch G, Ros E, Martínez-González M, et al. The effects of the Mediterranean diet on biomarkers of vascular wall inflammation and plaque vulnerability in subjects with high risk for cardiovascular disease. A randomized trial. PLoS One, 2014, 9(6): e100084. [Crossref]
16. Wang Y, Hao Q, Su L, Liu Y, Liu S, & Dong B. Adherence to the Mediterranean diet and the risk of frailty in old people: a systematic review and meta-analysis. J Nutr Health Aging, 2018, 22(5): 613-618. [Crossref]
17. Ghosh T, Rampelli S, Jeffery I, Santoro A, Neto M, Capri M, et al. Mediterranean diet intervention alters the gut microbiome in older people reducing frailty and improving health status: the NU-AGE 1-year dietary intervention across five European countries. Gut, 2020, 69(7): 1218-1228. [Crossref]
18. Micheli L, Bertini L, Bonato A, Villanova N, Caruso C, Caruso M, et al. Role of hydroxytyrosol and oleuropein in the prevention of aging and related disorders: focus on neurodegeneration, skeletal muscle dysfunction and gut microbiota. Nutrients, 2023, 15(7): 1767-1778. [Crossref]
19. Calabrò A, Aiello A, Silva P, Caruso C, Candore G, & Accardi G. Geroprotective applications of oleuropein and hydroxytyrosol through the hallmarks of ageing. Geroscience, 2025. [Crossref]
20. Salehi B, Mishra A, Nigam M, Sener B, Kilic M, Sharifi-Rad M, et al. Resveratrol: a double-edged sword in health benefits. Biomedicines, 2018, 6(3): 91-108. [Crossref]
21. Eggersdorfer M, & Wyss A. Carotenoids in human nutrition and health. Arch Biochem Biophys, 2018, 652: 18-26. [Crossref]
22. Calder P. Omega-3 fatty acids and inflammatory processes: from molecules to man. Biochem Soc Trans, 2017, 45(5): 1105-1115. [Crossref]
23. Liu J, Dong K, Deng Q, Zou Z, Chen S, Feng N, et al. Regulation of aging-related chronic diseases by dietary polyphenols: an updated overview. Curr Res Food Sci, 2025, 11: 101163. [Crossref]
24. Ahmed M. Targeting aging pathways with natural compounds: a review of curcumin, epigallocatechin gallate, thymoquinone, and resveratrol. Immun Ageing, 2025, 22(1): 28-41. [Crossref]
25. Forni C, Facchiano F, Bartoli M, Pieretti S, Facchiano A, D'Arcangelo D, et al. Beneficial role of phytochemicals on oxidative stress and age-related diseases. Biomed Res Int, 2019, 2019: 8748253. [Crossref]
26. Zhang H, & Tsao R. Dietary polyphenols, oxidative stress and antioxidant and anti-inflammatory effects. Curr Opin Food Sci, 2016, 8: 33-42. [Crossref]
27. Xu X, Pang Y, & Fan X. Mitochondria in oxidative stress, inflammation and aging: from mechanisms to therapeutic advances. Signal Transduct Target Ther, 2025, 10(1): 190-208. [Crossref]
28. Barcena M, Aslam M, Norman K, Ott C, & Ladilov Y. Role of AMPK and sirtuins in aging heart: basic and translational aspects. Aging Dis, 2024, 16(6): 3335-3360. [Crossref]
29. Guan Y, Li L, Yang R, Lu Y, & Tang J. Targeting mitochondria with natural polyphenols for treating neurodegenerative diseases: a comprehensive scoping review from oxidative stress perspective. J Transl Med, 2025, 23(1): 572-589. [Crossref]
30. Le Cosquer G, Vergnolle N, & Motta J. Gut microb-aging and its relevance to frailty aging. Microbes Infect, 2024, 26(3): 105309. [Crossref]
31. Escudero-Bautista S, Omaña-Covarrubias A, Nez-Castro A, López-Pontigo L, Pimentel-Pérez M, & Chávez-Mejía A. Impact of gut microbiota on aging and frailty: a narrative review of the literature. Geriatrics, 2024, 9(5): 110-121. [Crossref]
32. Tosti V, Bertozzi B, & Fontana L. Health benefits of the Mediterranean diet: metabolic and molecular mechanisms. J Gerontol A Biol Sci Med Sci, 2018, 73(3): 318-326. [Crossref]
33. Ney L, Wipplinger M, Grossmann M, Engert N, Wegner V, & Mosig A. Short chain fatty acids: key regulators of the local and systemic immune response in inflammatory diseases and infections. Open Biol, 2023, 13(3): 230014. [Crossref]
34. Qian X, Xie R, Liu X, Chen S, & Tang H. Mechanisms of short-chain fatty acids derived from gut microbiota in Alzheimer's disease. Aging Dis, 2022, 13(4): 1252-1266. [Crossref]
35. Cardona F, Andrés-Lacueva C, Tulipani S, Tinahones FJ, & Queipo-Ortuño MI. Benefits of polyphenols on gut microbiota and implications in human health. J Nutr Biochem, 2013, 24(8): 1415-1422. [Crossref]
36. Ticinesi A, Lauretani F, Tana C, Nouvenne A, Ridolo E, & Meschi T. Exercise and immune system as modulators of intestinal microbiome: implications for the gut-muscle axis hypothesis. Exerc Immunol Rev, 2019, 25: 8-20.
37. Cryan J, O'Riordan K, Cowan S, Sandhu K, Bastiaanssen T, Boehme M, et al. The microbiota-gut-brain axis. Physiol Rev, 2019, 99(4): 1877-2013. [Crossref]
38. Cruz-Jentoft A, Bahat G, Bauer J, Boirie Y, Bruyère O, Cederholm T, et al. Sarcopenia: revised European consensus on definition and diagnosis. Age Ageing, 2019, 48(1): 16-31. [Crossref]
39. Volkert D, Beck A, Cederholm T, Cruz-Jentoft A, Hooper L, Kiesswetter E, et al. ESPEN practical guideline: clinical nutrition and hydration in geriatrics. Clin Nutr, 2022, 41(4): 958-989. [Crossref]
40. Calvani R, Picca A, Coelho-Júnior H, Tosato M, Marzetti E, & Landi F. Diet for the prevention and management of sarcopenia. Metabolism, 2023, 146: 155637. [Crossref]
41. Soysal P, Stubbs B, Lucato P, Luchini C, Solmi M, Peluso R, et al. Inflammation and frailty in the elderly: a systematic review and meta-analysis. Ageing Res Rev, 2016, 31: 1-8. [Crossref]
42. Justice J, Nambiar A, Tchkonia T, LeBrasseur N, Pascual R, Hashmi S, et al. Senolytics in idiopathic pulmonary fibrosis: results from a first-in-human, open-label, pilot study. EBioMedicine, 2019, 40: 554-563. [Crossref]
43. Muthamil S, Kim H, Jang H, Lyu J, Shin U, Go Y, et al. Biomarkers of cellular senescence and aging: current state-of-the-art, challenges and future perspectives. Adv Biol, 2024, 8(9): e2400079. [Crossref]
44. Natarajan D, Plakkot B, Tiwari K, Ekambaram S, Wang W, Rudolph M, et al. Chronic β3-AR stimulation activates distinct thermogenic mechanisms in brown and white adipose tissue and improves systemic metabolism in aged mice. Aging Cell, 2024, 23(12): e14321. [Crossref]
45. Justice J, Ferrucci L, Newman A, Aroda V, Bahnson J, Divvers J, et al. A framework for selection of blood-based biomarkers for geroscience-guided clinical trials: report from the TAME Biomarkers Workgroup. GeroScience, 2018, 40(5-6): 419-436. [Crossref]
46. Castro-Barquero S, Lamuela-Raventós R, Doménech M, & Estruch R. Relationship between Mediterranean dietary polyphenol intake and obesity. Nutrients, 2018, 10(10): 1523-1536. [Crossref]