Open Access | Commentary
This work is licensed under a Creative Commons Attribution-ShareAlike 4.0 International License.
The association of post-traumatic stress disorder with accelerated aging
* Corresponding author: Anton R. Kiselev
Mailing address: Coordinating Center for Fundamental Research,
National Medical Research Center for Therapy and Preventive
Medicine, Moscow 101990, Russia.
Email: antonkis@list.ru
Received: 22 May 2026 / Accepted: 22 June 2026 / Published: 30 June 2026
DOI: 10.31491/APT.2026.06.223
Abstract
Post-traumatic stress disorder (PTSD) is increasingly recognized as a multisystem condition associated with accelerated biological aging. However, the heterogeneity of aging trajectories and causal mechanisms remain poorly defined. This commentary critically synthesizes evidence linking PTSD to telomere attrition, epigenetic age acceleration, chronic inflammation, and increased dementia risk, while emphasizing that most data are cross-sectional and causal inference is limited. We propose a working hypothesis of four hypothetical aging subtypes (telomere/inflammaging-dominant, epigenetic-dominant, neurodegeneration-dominant, and resilient) as a heuristic framework to guide future research. We argue that without recognizing this heterogeneity, translational efforts will remain suboptimal. The priority for future studies is longitudinal multi-biomarker designs with cluster analyses to empirically validate or refute the proposed subtypes. Effective interventions may mitigate these effects, but direct evidence for reversibility of biological aging markers is currently lacking.
Keywords
Post-traumatic stress disorder, accelerated aging, epigenetic clock, inflammaging, dementia
Introduction
The conceptualization of post-traumatic stress disorder (PTSD) is arguably undergoing a paradigm shift, moving beyond narrow psychiatric confines to be redefined as a chronic, multisystem pathology [1]. Current data points toward a profound disruption of the neuroendocrine-immune axis, leading to a cumulative allostatic load [2], a process that is further illuminated by recent research on cognitive appraisal and coping strategies in patients with chronic coronary syndrome and psychological distress [3]. This systemic dysregulation frequently acts as a precursor to severe somatic comorbidities, which fundamentally underscore the disorder's capacity to shorten life expectancy [4]. Consequently, addressing PTSD through a purely clinical-psychological lens appears increasingly insufficient, necessitating a holistic medical framework to mitigate its far-reaching physiological toll.
Numerous meta-analyses have confirmed that PTSD is associated with an increased risk of cardiovascular disease, type 2 diabetes, and dementia [4-6]. However, the critical unanswered question is not whether PTSD accelerates aging, but how and for whom. The striking inter-individual variability in aging trajectories suggests that PTSD-related biological aging is not a uniform process. This commentary aims to: (i) critically synthesize the evidence for PTSD-accelerated aging with a focus on heterogeneity; (ii) propose a heuristic four-subtype framework as a testable hypothesis; and (iii) identify key methodological gaps that must be addressed to validate this framework. We argue that without recognizing this heterogeneity, translational efforts will remain suboptimal.
Established associations of PTSD: a critical synopsis
Multiple lines of evidence support the association between PTSD and accelerated biological aging. Individuals with PTSD consistently exhibit shorter telomeres compared to trauma-exposed controls without PTSD [7]. Epigenetic age acceleration, measured by DNA methylation (DNAm) clocks such as GrimAge and Horvath clock, has been demonstrated in veteran cohorts and linked to reduced neural integrity [8, 9]. Oxidative stress and mitochondrial dysfunction, comprehensively reviewed by Miller and Sadeh [10], represent another mechanistic pathway,
though evidence remains largely cross-sectional.
PTSD is also consistently associated with a chronic low-grade inflammatory state. Landmark meta-analyses have found significantly elevated levels of interleukin-6, tumor necrosis factor-α, and C-reactive protein in individuals with PTSD compared to healthy controls [11, 12]. Wolf and Morrison reviewed evidence linking these inflammatory changes to downstream cardiometabolic disease, suggesting a mechanistic pathway from traumatic stress to inflammation to accelerated biological aging [5].
Recent Mendelian randomization analyses have demonstrated that elevated levels of specific inflammatory cytokines, namely stem cell factor and interleukin-4, are causally associated with reduced PTSD risk, implicating the transforming growth factor β (TGF-β) signaling pathway and molecular mediators such as POGZ and LRIG2 as protective nodes [13]. These findings mark a paradigm shift: PTSD is not merely accompanied by immune dysregulation, but specific inflammatory profiles may causally influence disease susceptibility.
Neuroimaging studies have documented reduced hippocampal, prefrontal cortical, and anterior cingulate volumes in PTSD, with duration of PTSD predicting progressive hippocampal gray matter loss [14]. In service members with PTSD and mild traumatic brain injury, age-accelerated reductions in cortical surface area were demonstrated [15]. The epidemiological evidence for PTSD as a risk factor for dementia is robust [6, 16, 17].
Heterogeneity of aging trajectories in PTSD
The most frequently identified trajectories of response to potentially traumatic events include: the resilience trajectory, the recovery trajectory, the chronic dysfunction trajectory, and the delayed onset trajectory [18, 19]. The resilience trajectory is the most common and is characterized by the absence of a significant increase in symptoms. The recovery trajectory involves an initial increase in symptomatology followed by a gradual reduction. In chronic dysfunction, there is a persistent retention of PTSD symptoms. In the delayed onset trajectory, symptoms emerge months or years later, which is of particular interest to geriatric psychiatry as it may be associated with age-related changes and stressors of later life [20].
Research shows that the course of PTSD in older adults can vary significantly depending on the age at which the trauma occurred. Two main scenarios are distinguished: early-life trauma with symptoms persisting or recurring in old age [20], and new trauma occurring in old age leading to de novo PTSD [21]. The significant prevalence of PTSD and other mental health issues has also been documented in other populations under high stress, such as medical students during the COVID-19 pandemic [22]. A 10-year longitudinal study of Holocaust survivors found that 10% of participants who did not have PTSD at the first assessment developed delayed PTSD by the second assessment, indicating the reality of a late onset of the disorder [20].
The clinical heterogeneity of PTSD raises the possibility that biological aging trajectories also differ across individuals. Building on PTSD pathways, the followed four-subtype framework maybe represent the heterogeneity of accelerated aging in PTSD. To date, no study has directly tested this four-subtype classification using cluster analysis or latent profile analysis in a sample with comprehensive biomarker data. Here, we propose a hypothetical four-subtype framework to guide future research, not as a validated taxonomy (Figure 1).
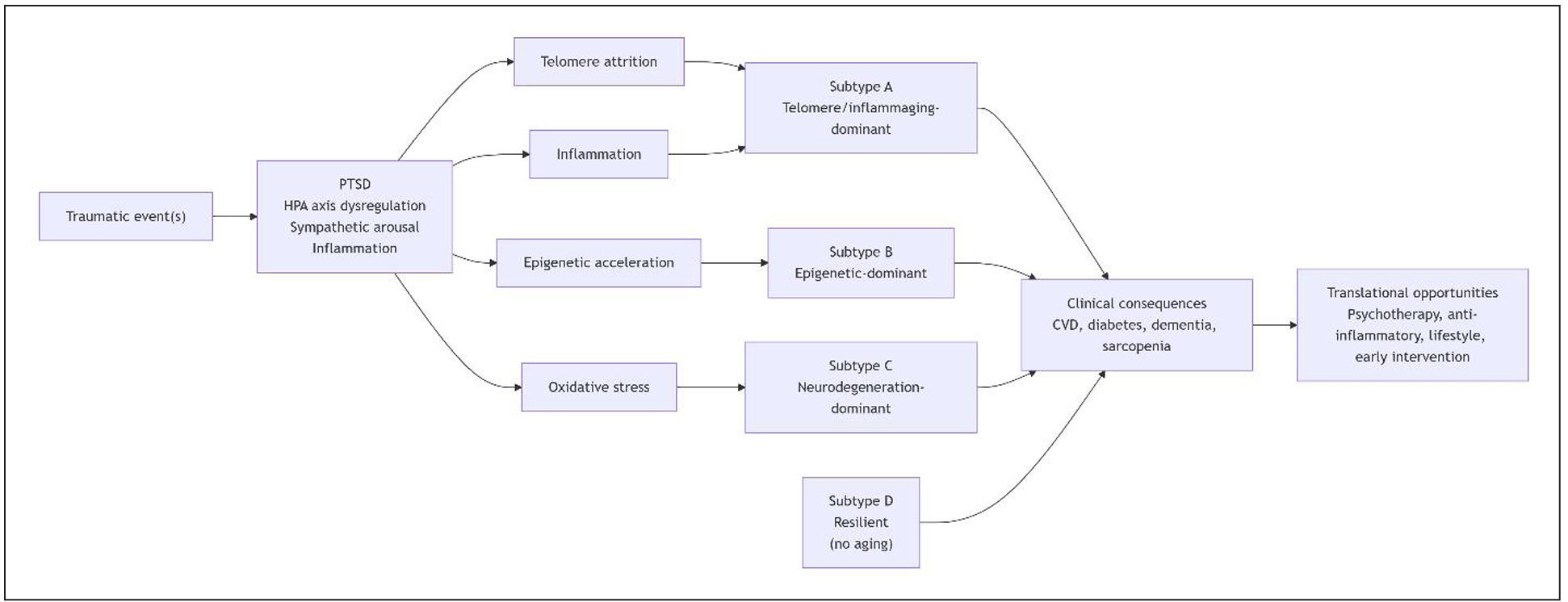
Figure 1. Hypothetical framework linking post‑traumatic stress disorder (PTSD) to accelerated biological aging and proposed heterogeneity of aging trajectories.
Subtype A: telomere-driven/inflammaging-dominant
Strong evidence supports the existence of a PTSD subgroup characterized by pronounced telomere shortening and elevated inflammation. Miller and Sadeh proposed a theoretical model whereby chronic PTSD potentiates oxidative stress (OXS), which in turn drives telomere erosion and cellular senescence, forming a self-perpetuating cycle [10]. This model aligns well with Subtype A as a distinct mechanistic pathway. However, the extent to which this pathway is separable from other aging mechanisms (e.g., epigenetic aging) remains unclear, as these processes are likely interconnected.
Subtype B: epigenetic clock acceleration-dominant (without rapid neurodegeneration)
Multiple studies have established that PTSD is associated with accelerated epigenetic aging [8, 9, 23, 24]. The differentiation from Subtype A is conceptually plausible—epigenetic clocks capture different biological processes than telomere length—though in practice there is considerable overlap. The "without rapid neurodegeneration" qualifier is more difficult to validate given that Wolf et al. did find that DNAm age acceleration was associated with reduced white matter integrity [8]. However, the epigenetic aging pathway may precede overt structural brain changes.
Subtype C: neurodegeneration-dominant (brain structure decline, cognitive impairment)
The evidence linking PTSD to neurodegeneration and dementia risk is substantial [6, 10, 15, 25, 26]. This subtype may represent the end-stage of accelerated aging processes that begin with molecular changes (Subtypes A and B) and eventually manifest as structural brain decline.
Subtype D: resilient (no accelerated aging despite PTSD)
This is the least studied of the four subtypes but has emerging empirical support. The concept of a resilient subtype is consistent with the observation that not all individuals with PTSD develop accelerated aging: there is considerable inter-individual variability in biomarker profiles [4, 5]. Positive mental health has been shown to moderate the association between PTSD symptoms and subjective accelerated aging [27]. The evidence for a distinct resilient subtype is preliminary but conceptually important. However, further research is needed to determine whether this represents a true subtype (i.e., stable trait-like resistance to biological aging) or rather reflects state-dependent factors such as differential treatment response, symptom fluctuation, or compensatory biological mechanisms.
It is crucial to acknowledge that this four-subtype framework remains speculative. The current evidence base is severely limited by: (a) cross-sectional designs that cannot establish temporality; (b) residual confounding from early-life adversity and lifestyle factors; (c) overrepresentation of male veteran cohorts; and (d) inconsistent results across different epigenetic clocks. These limitations preclude any clinical application of our model at present.
The proposed subtypes may represent different stages or facets of a common accelerated aging cascade rather than discrete entities. It is plausible that Subtypes A and B represent earlier molecular stages of accelerated aging, while Subtype C reflects later-stage structural and cognitive consequences. Longitudinal studies tracking all biomarkers simultaneously are needed. We urge readers to treat this as a heuristic device, not a clinical classification.
The heterogeneity of PTSD aging trajectories has important clinical implications. First, diagnostic screening for PTSD in elderly patients should take into account the possibility of delayed onset and atypical clinical presentations, which may be masked by somatic
complaints or cognitive impairment [4]. Second, therapeutic interventions need to be adapted based on the patient's age, duration of the disorder, and cognitive status.
Translational opportunities
If our subtype framework proves valid, it would have direct translational implications. For Subtype A (inflammaging-dominant), anti-inflammatory or antioxidant strategies might be prioritized; for Subtype C (neurodegeneration-dominant), neuroprotective interventions would be relevant. Encouragingly, longitudinal evidence suggests that changes in PTSD symptom severity correlate with changes in DNAm GrimAge acceleration [9, 28], indicating that effective treatment might slow further biological aging. However, no study has yet demonstrated reversibility of aging markers, and the optimal intervention type likely depends on the predominant biological pathway in each individual. This underscores the urgent need for subtype-specific intervention trials.
Conclusions
In conclusion, the convergence of molecular, structural, and clinical evidence strongly suggests that PTSD alters aging trajectories, but this process is likely heterogeneous. Our proposed four-subtype framework offers a heuristic tool to guide future research, not a validated taxonomy. The priority for the field is clear: longitudinal multi-biomarker studies with cluster analyses are urgently needed to empirically validate or refute these subtypes. Only then can we move toward personalized interventions that target the specific aging pathways activated in each individual with PTSD. Until such data emerge, claims about reversibility or precision treatment remain premature.
Declarations
Availability of data and materials
Not applicable.
Financial support and sponsorship
None.
Conflicts of interests
Not applicable.
Consent for publication
Not applicable.
Funding
This study was supported by the Russian Science Foundation (Project No. 25-44-10019).
AI and AI-assisted tools statement
During the preparation of this work, the author used ChatGPT to improve readability and phrasing. After using this tool, the author reviewed and edited the content as needed and takes full responsibility for the final content.
References
1. McFarlane A. Post-traumatic stress disorder is a systemic illness, not a mental disorder: is Cartesian dualism dead? Med J Aust, 2017, 206(6): 248-249. [Crossref]
2. Juster R, McEwen B, & Lupien S. Allostatic load biomarkers of chronic stress and impact on health and cognition. Neurosci Biobehav Rev, 2010, 35(1): 2-16. [Crossref]
3. Sumin A, Shcheglova A, Anchkova M, Fedorova D, & Prokashko I. Psychological distress in patients with chronic coronary syndrome: features of coping strategies and cognitive appraisal in depression and Type D personality. Russ Open Med J, 2025, 14: e0408. [Crossref]
4. Lohr J, Palmer B, Eidt C, Aailaboyina S, Mausbach B, Wolkowitz O, et al. Is post-traumatic stress disorder associated with premature senescence? A review of the literature. Am J Geriatr Psychiatry, 2015, 23(7): 709-725. [Crossref]
5. Wolf E, & Morrison F. Traumatic stress and accelerated cellular aging: from epigenetics to cardiometabolic disease. Curr Psychiatry Rep, 2017, 19(10): 75-88. [Crossref]
6. Neylan T. Post-traumatic stress disorder and neurodegeneration. Am J Geriatr Psychiatry, 2020, 28(1): 61-63. [Crossref]
7. O'Donovan A, Epel E, Lin J, Wolkowitz O, Cohen B, Maguen S, et al. Childhood trauma associated with short leukocyte telomere length in posttraumatic stress disorder. Biol Psychiatry, 2011, 70(5): 465-471. [Crossref]
8. Wolf E, Logue M, Hayes J, Sadeh N, Schichman S, Stone A, et al. Accelerated DNA methylation age: associations with PTSD and neural integrity. Psychoneuroendocrinology, 2016, 63: 155-162. [Crossref]
9. Yang R, & Wu G. DNA methylation clock associated with age-related illnesses is accelerated in PTSD. Neuropsychopharmacology, 2021, 46(1): 225-226. [Crossref]
10. Miller M, & Sadeh N. Traumatic stress, oxidative stress and post-traumatic stress disorder: neurodegeneration and the accelerated-aging hypothesis. Mol Psychiatry, 2014, 19(11): 1156-1162. [Crossref]
11. Passos I, Vasconcelos-Moreno M, Costa L, Kunz M, Brietzke E, Quevedo J, et al. Inflammatory markers in post-traumatic stress disorder: a systematic review, meta-analysis, and meta-regression. Lancet Psychiatry, 2015, 2(11): 1002-1012. [Crossref]
12. Yang J, & Jiang W. Immune biomarkers alterations in post-traumatic stress disorder: a systematic review and meta-analysis. J Affect Disord, 2020, 268: 39-46. [Crossref]
13. Li Y, Xu B, & Chen Z. Causal relationship between inflammatory cytokines and posttraumatic stress disorder: a Mendelian randomization study and potential mechanism analysis. Eur J Psychotraumatol, 2025, 16(1): 2494480. [Crossref]
14. Felmingham K, Williams L, Whitford T, Falconer E, Kemp A, Peduto A, et al. Duration of posttraumatic stress disorder predicts hippocampal grey matter loss. Neuroreport, 2009, 20(16): 1402-1406. [Crossref]
15. Santhanam P, Wilson S, Mulatya C, Oakes T, & Weaver L. Age-accelerated reduction in cortical surface area in United States service members and veterans with mild traumatic brain injury and post-traumatic stress disorder. J Neurotrauma, 2019, 36(20): 2922-2929. [Crossref]
16. Mohlenhoff B, O'Donovan A, Weiner M, & Neylan T. Dementia risk in posttraumatic stress disorder: the relevance of sleep-related abnormalities in brain structure, amyloid, and inflammation. Curr Psychiatry Rep, 2017, 19(11): 89-102. [Crossref]
17. Günak M, Billings J, Carratu E, Marchant N, Favarato G, & Orgeta V. Post-traumatic stress disorder as a risk factor for dementia: systematic review and meta-analysis. Br J Psychiatry, 2020, 217(5): 600-608. [Crossref]
18. Dickstein B, Suvak M, Litz B, & Adler A. Heterogeneity in the course of posttraumatic stress disorder: trajectories of symptomatology. J Trauma Stress, 2010, 23(3): 331-339. [Crossref]
19. Mancini A, & Bonanno G. Beyond resilience and PTSD: mapping the heterogeneity of responses to potential trauma. Psychol Trauma, 2012, 4(1): 74-83. [Crossref]
20. Yehuda R, Schmeidler J, Labinsky E, Bell A, Morris A, Zemelman S, et al. Ten-year follow-up study of PTSD diagnosis, symptom severity and psychosocial indices in aging holocaust survivors. Acta Psychiatr Scand, 2009, 119(1): 25-34. [Crossref]
21. Jakel R. Posttraumatic stress disorder in the elderly. Psychiatr Clin North Am, 2018, 41(1): 165-175. [Crossref]
22. Fang L. A study of the mental health status of Chinese medical students at risk of COVID-19 infection. Russ Open Med J, 2026, 15: e0105. [Crossref]
23. Kuan P, Ren X, Clouston S, Yang X, Jonas K, Kotov R, et al. PTSD is associated with accelerated transcriptional aging in World Trade Center responders. Transl Psychiatry, 2021, 11(1): 311-325. [Crossref]
24. Verhoeven J, Yang R, Wolkowitz O, Bersani F, Lindqvist D, Mellon S, et al. Epigenetic age in male combat-exposed war veterans: associations with posttraumatic stress disorder status. Mol Neuropsychiatry, 2018, 4(2): 90-99. [Crossref]
25. Yaffe K, Vittinghoff E, Lindquist K, Barnes D, Covinsky K, Neylan T, et al. Posttraumatic stress disorder and risk of dementia among US veterans. Arch Gen Psychiatry, 2010, 67: 608-613. [Crossref]
26. Wang T, Wei H, Liou Y, Su T, Bai Y, Tsai S, et al. Risk for developing dementia among patients with posttraumatic stress disorder: a nationwide longitudinal study. J Affect Disord, 2016, 205: 306-310. [Crossref]
27. Palgi Y. Positive mental health moderates the association between PTSD symptoms and subjective accelerated aging among older adults. Int Psychogeriatr, 2020, 32(7): 885-889. [Crossref]
28. Zhao X, Katrinli S, McCormick B, Miller M, Nugent N, Wani A, et al. PTSD and epigenetic aging: a longitudinal meta-analysis. Psychol Med, 2025, 55: e142. [Crossref]