Open Access | Review
This work is licensed under a Creative Commons Attribution-ShareAlike 4.0 International License.
Contemporary surgical management of urolithiasis: a narrative review
* Corresponding author: Miguel Angel Arrabal Polo
Mailing address: Servicio de Urología, Hospital Universitario Clínico San Cecilio Avda. del Conocimiento s/n, 18016 Granada, Spain.
Email: arrabalp29@gmail.com
Received: 11 May 2026 / Revised: 05 June 2026 / Accepted: 10 June 2026 / Published: 30 June 2026
DOI: 10.31491/UTJ.2026.06.060
Abstract
Urolithiasis is among the most prevalent urological conditions worldwide, with a rising incidence driven by obesity, metabolic syndrome, and climate-related factors, and an estimated global annual expenditure exceeding USD 5.3 billion. This is a narrative review of the literature. Relevant publications were identified through searches of PubMed/MEDLINE, EMBASE, and the Cochrane Library (last searched January 2025) using terms related to surgical management of kidney and ureteral stones, with priority given to systematic reviews, meta-analyses, randomized controlled trials, and current European Association of Urology (EAU) and American Urological Association (AUA) clinical practice guidelines. The review synthesizes current evidence on their surgical management, encompassing advances in laser lithotripsy technology, the evolving role of retrograde intrarenal surgery (RIRS), percutaneous nephrolithotomy (PCNL) techniques, and management in special clinical situations including horseshoe kidney (HK), pelvic ectopic kidney, solitary kidney, pregnancy, and pediatric patients. Treatment selection is governed by stone size, location, composition, patient anatomy, comorbidities, and local surgical expertise, as outlined in current EAU and AUA guidelines. Three key clinical messages emerge from the reviewed literature: (i) RIRS has become a widely adopted minimally invasive option for renal stones up to 20 mm as a primary indication, with selected larger stones in high-morbidity patients (stone-free rates [SFRs] consistently > 80% for 10–20 mm stones), though treatment should be individualized rather than modality-driven; (ii) PCNL remains the reference standard for large and staghorn stones (SFR up to 95% in a single session); (iii) newer laser platforms, particularly the thulium fiber laser (TFL), show promising technical advantages whose definitive clinical significance relative to modern holmium:YAG (Ho:YAG) systems requires confirmation through larger prospective comparative studies. In special clinical situations, RIRS is preferred in the solitary kidney and pregnancy (SFR 80–90%), while PCNL or RIRS are selected for HK according to stone burden (SFR 80–95% and 60–100%, respectively). Robust randomized trials and standardized outcome reporting remain necessary to guide future evidence-based practice.
Keywords
Urolithiasis, kidney stones, ureteroscopy, percutaneous nephrolithotomy, laser lithotripsy, horseshoe kidney
Introduction
Urolithiasis is a globally prevalent urological disease, with prevalence estimates ranging from 1% to 13% depending on geographic, dietary, climatic, and genetic factors [1]. In developed countries, renal stone prevalence exceeds 10%, and increases of more than 37% over the past two decades have been reported in some regions [1]. These figures, largely derived from North American and European data from the 2000s and early 2010s, reflect epidemiological trends documented prior to the publication of more recent surveillance studies; the underlying drivers (obesity, metabolic syndrome, global warming) continue to support an upward trajectory, though precise updated global estimates remain heterogeneous across regions. The disease carries a substantial economic burden, accounting for an estimated USD 5.3 billion in annual global expenditure and constituting the second most costly urological condition [2]. Rising rates of obesity, diabetes, metabolic syndrome, and global warming are considered primary drivers of this epidemiological trend [1, 2].
The management of urolithiasis has undergone a fundamental transformation over the past four decades. Open surgery, once the mainstay of treatment, has been largely replaced by minimally invasive endourological techniques: extracorporeal shock wave lithotripsy (ESWL), retrograde intrarenal surgery (RIRS) using a flexible ureterorenoscope (fURS), and percutaneous nephrolithotomy (PCNL). These modalities are now recommended as standard treatments by both the European Association of
Urology (EAU) and American Urological Association (AUA) guidelines [1, 3]. Despite this progress, clinically important questions persist regarding optimal modality selection, particularly for intermediate stone sizes (10–20 mm, for which both RIRS and PCNL have overlapping guideline indications and comparative outcomes remain debated), anatomically complex presentations (including horseshoe kidney (HK), calyceal diverticula, and lower pole stones with unfavorable infundibulopelvic angles, where standard endoscopic approaches may achieve suboptimal stone-free rates (SFRs)), and special clinical populations (specifically patients with a solitary kidney requiring maximum safety, pregnant women in whom procedural timing and radiation exposure must be minimized, and pediatric patients with distinct anatomical and metabolic considerations). In addition, the relative merits of competing technological platforms remain incompletely established [1]. Concurrent advances in laser technology, including high-power Ho:YAG systems, Moses modulation technology, the thulium fiber laser (TFL), and the pulsed thulium:YAG (p-Tm:YAG) laser, have further expanded the efficacy and safety of endoscopic stone treatment, although their comparative clinical value is still being defined [4, 5].
The aim of the present review is to provide a structured, clinically oriented synthesis of current evidence on the surgical management of urolithiasis, with emphasis on
technological advances, guideline-based treatment indications, and decision-making in special clinical situations.
Methods
A narrative review of the literature was conducted. Relevant publications were identified through searches of PubMed/MEDLINE, EMBASE, and the Cochrane Library (last searched January 2025) using the following search terms: “kidney stones surgical treatment”, “kidney stones management”, “kidney stones in horseshoe kidney”, “kidney stones pelvic kidney”, “kidney stones in renal anomalies”, and “ureteral stones management”. Searches were not restricted by language; publications from 2014 onwards were prioritized, with earlier landmark studies included where relevant. Systematic reviews, meta-analyses, and randomized controlled trials (RCTs) were given priority, followed by high-quality comparative observational studies and the most recent versions of the EAU (2026) and AUA (2026) clinical practice guidelines [1, 3]. Given the narrative nature of the review, no formal PRISMA-guided systematic selection process was applied; the objective was to provide a clinically oriented synthesis of the most relevant and contemporary evidence across the main surgical modalities and special clinical scenarios, rather than an exhaustive systematic appraisal. Evidence levels and recommendation grades are assigned throughout the text according to the Oxford Centre for Evidence-Based Medicine (Oxford CEBM) 2011 Levels of evidence (Levels 1–5) and corresponding Grades of Recommendation (A–D), where applicable. Grade A reflects consistent Level 1 evidence (systematic reviews and meta-analyses of RCTs); Grade B reflects Level 2–3 evidence (systematic reviews of cohort or case-control studies); Grade C reflects Level 4 evidence (case series); and Grade D reflects Level 5 (expert opinion). Where recommendations derive from formal clinical practice guidelines (EAU or AUA), this is stated explicitly.
Laser technology in stone lithotripsy
The introduction of intracorporeal laser lithotripsy was a pivotal advance in endoscopic stone treatment. Laser platforms have undergone continuous development aimed at improving ablation efficiency, reducing stone retropulsion, and minimizing thermal injury to adjacent tissues [4].
Holmium:YAG laser
The Ho:YAG laser, operating at a wavelength of 2120 nm, has been considered the reference standard for intracorporeal lithotripsy since the 1990s and represents the platform on which the broadest clinical evidence base has been built [4]. Its mechanism relies on photothermal ablation, with high water absorption limiting thermal penetration to approximately 400 μm. Two principal operational modes are employed: fragmentation (high-energy, low-frequency pulses) and dusting (low-energy, high-frequency pulses). Despite its versatility across stone compositions, recognized limitations include a minimum fiber diameter of 150 µm, heat generation at high-power settings with low irrigation flow, and a fragmentation efficiency plateau at frequencies above approximately 61.6 Hz [4].
Moses technology
Commercially introduced in 2017, Moses technology (Lumenis) modulates the Ho:YAG pulse into two sequential sub-pulses: the first creates a vapor channel through the surrounding fluid (the “Moses effect”) and the second travels through this channel to interact more directly with the stone target, thereby reducing energy loss in the fluid medium [4]. This modulation has been shown in experimental settings to improve energy delivery efficiency and reduce stone retropulsion compared with unmodulated Ho:YAG. The Moses 2.0 system operates at up to 120 Hz, extending its application range. Robust randomized comparative trials against contemporary Ho:YAG systems remain limited, and the clinical significance of the observed advantages requires further validation [4].
TFL
The TFL operates at a wavelength of 1940 nm and has shown promising technical and early clinical advantages over conventional Ho:YAG platforms [4, 5]. Its water absorption coefficient is approximately 4–5 times higher than that of Ho:YAG, and its pulse profile is more uniform and focused. The TFL can be transmitted through fibers as small as 50–150 µm, facilitating access to anatomically challenging lower pole calyces and enabling dusting strategies with minimal retropulsion. In vitro and early in vivo studies demonstrate favorable ablation rates across multiple stone compositions; however, the definitive clinical position of TFL relative to contemporary Ho:YAG platforms, in terms of SFRs, operative time, and complication profiles across the full range of clinical scenarios, remains to be established through larger prospective comparative studies [4, 5].
p-Tm:YAG laser
The p-Tm:YAG laser represents the most recent addition to the lithotripsy armamentarium and may occupy a middle ground between the Ho:YAG and TFL in terms of
peak power and pulse stability [5]. Early clinical series combining p-Tm:YAG with fURS and mini-PCNL report high SFRs with low complication rates, though available evidence derives from small, single-center experiences. Larger prospective studies are required before definitive clinical recommendations can be formulated [5].
Although newer laser platforms may improve ablation efficiency and reduce retropulsion in selected settings, the clinical significance of these differences remains context-dependent, and technology alone cannot substitute for careful patient selection, procedural planning, and surgical expertise [4, 5].
Surgical treatment of renal stones
Table 1 provides a comparative overview of the main surgical modalities for urolithiasis, including their primary indications, principal strengths, main limitations, typical complications, and recommended clinical scenarios with evidence grades to facilitate treatment selection at the point of care.
Table 1.
Main surgical modalities for urolithiasis: indications, principal strengths, limitations, typical complications, and recommended clinical scenario.
| Modality | Primary indications | Principal strengths | Main limitations | Typical complications | Recommendation grade (Oxford CEBM 2011) |
|---|---|---|---|---|---|
| ESWL | Renal stones ≤ 20 mm with favorable anatomy; ureteral stones ≤ 10 mm | Non-invasive; outpatient; no general anesthesia required | Lower SFR for large/hard stones, lower pole, obesity; high retreatment rate | Hematuria (~17%); steinstrasse (~4%); symptomatic renal hematoma (~0.21%) [2] | A |
| RIRS (fURS) | Renal stones ≤ 20 mm; ureteral stones; selected larger stones in high-morbidity patients | Minimally invasive; no percutaneous access; broad anatomical reach; single-use scopes available | Multiple sessions may be needed for large stones; retropulsion risk; equipment-dependent | Urosepsis (1–6.6%); hematuria; fever; UTI (predominantly CD grade I–II) [6] | A |
| Standard PCNL (24–30 Fr) | Renal stones > 20 mm; staghorn calculi; stones refractory to RIRS or ESWL | Highest single-session SFR for large stones (up to 95%) | Percutaneous access; general anesthesia; risk with supracostal approach | Transfusion (0–17%); urosepsis (1–6%); pneumothorax; perirenal hematoma [6] | A |
| Mini-PCNL (10–20 Fr) | Renal stones up to 30 mm; lower pole stones; ESWL failures; pediatric patients | Comparable SFR to standard PCNL ≤ 30 mm; lower blood loss; shorter hospital stays; less pain | Longer operative time than standard PCNL; higher intrarenal pressure concerns | Similar to standard PCNL but with reduced transfusion rate and less postoperative pain [3] | A |
| Laparoscopic ureterolithotomy (LU) | Large proximal ureteral stones refractory to URS or PCNL; concomitant reconstructive surgery | Higher initial SFR than PCNL for large PUS (OR 3.26; P = 0.004); lower transfusion rate [7] | Longer operative time; laparoscopic expertise required; not first-line endoscopic option | General surgical complications; ureteral injury; urinoma [7] | B |
| Open surgery | Exceptional cases: failed minimally invasive approaches; complex anatomy with concomitant reconstruction | Complete access; no instrument limitations | Highest morbidity; prolonged recovery; reserved for rare cases | Wound complications; significant bleeding; prolonged hospitalization | D |
Notes: ESWL: extracorporeal shock wave lithotripsy; ALARA: as low as reasonably achievable; CD: Clavien-Dindo; fURS: flexible ureterorenoscopy; PCNL: percutaneous nephrolithotomy; PUS: proximal ureteral stones; RIRS: retrograde intrarenal surgery; SFR: stone-free rate; UTI: urinary tract infection; URS: ureteroscopy.
ESWL
ESWL remains a recommended first-line treatment for renal stones ≤ 20 mm with favorable anatomical and stone characteristics, as specified in both EAU and AUA guidelines [1, 3] (Oxford Level 1a; Grade A). Its principal advantages are non-invasiveness, outpatient delivery, and absence of general anesthesia requirement. SFRs decline significantly for stones > 10 mm, high-density stones (900–1000 Hounsfield units on non-contrast CT), lower pole calculi, and patients with obesity or anatomical anomalies [1]. Strategies to optimize outcomes include a slow shockwave delivery rate, adequate patient hydration, and adjuvant alpha-blocker therapy after treatment [1, 3]. When these favorable conditions are absent, RIRS or PCNL should be considered as primary options.
RIRS
RIRS has become a widely adopted minimally invasive
option for renal stones across a broad size range, particularly in patients in whom a reduced morbidity profile is prioritized [8, 9]. Advances in flexible ureteroscope technology, including digital optics, improved active deflection (> 270°), reduced shaft diameters (≤ 7.5 Fr), and the availability of ureteral access sheaths (UAS) have progressively expanded its clinical application [8, 10, 11].
Single-use fURS instruments have further broadened access to this technology, demonstrating comparable performance to reusable devices while eliminating repair costs
and sterilization constraints [8].
For renal stones of 10–20 mm, overall SFRs following single or multiple sessions are consistently high across contemporary series [9] (Oxford Level 1a; Grade A). For stones > 20 mm, RIRS may require multiple sessions but generally maintains a more favorable complication profile than PCNL; treatment selection should be individualized according to stone burden, collecting system anatomy, patient comorbidities, and local surgical expertise rather than modality preference alone [1, 3, 9]. Complications are predominantly Clavien-Dindo (CD) grade I–II; major complications (CD ≥ III) are infrequent, with urosepsis reported in 1–6.6% of cases across published series [6]. This range reflects the heterogeneity of the included studies in Grosso et al. [6], which pooled data from over 14,000 patients across studies with variable patient populations, surgical volumes, and antibiotic prophylaxis protocols; the upper end (6.6%) derives from series in which preexisting urinary tract infection or ureteral dilation were not systematically excluded. Recognized anatomical factors unfavorable for RIRS include an acute infundibulopelvic angle, long infundibular length, narrow calyceal neck, congenital renal anomalies, and calyceal diverticular stones [12].
PCNL
PCNL remains the reference standard for renal stones > 20 mm and staghorn calculi, achieving SFRs approaching 95% in a single session for these indications [1, 3] (Oxford Level 1a; Grade A). Standard PCNL employs a tract dilated to 24–30 Fr under fluoroscopic or ultrasound guidance, typically in the prone position. Mini-PCNL (10–20 Fr) achieves comparable SFRs to standard PCNL for stones up to approximately 30 mm, with lower blood loss, reduced postoperative pain, and shorter hospital stay, though at the cost of longer operative time [3]. Ultrasound-guided access reduces radiation exposure and offers comparable safety to fluoroscopy-guided access in experienced hands [1]. Preoperative planning using three-dimensional printed models of the collecting system represents a promising adjunctive tool for complex cases, potentially reducing the number of required tracts and improving puncture accuracy [13].
Laparoscopic, robotic, and open surgery
Open and laparoscopic/robotic surgery currently occupy a very limited role, reserved for cases in which minimally invasive techniques have failed, are anatomically unfeasible, or are combined with a concomitant reconstructive procedure such as pyeloplasty [1, 3]. Laparoscopic ureterolithotomy achieves higher initial SFRs than PCNL for large proximal ureteral stones in meta-analytic data (OR 3.26; 95% CI 1.45–7.31; P = 0.004) with a lower transfusion rate, though at the cost of significantly longer operative times, and should be reserved for cases in which endoscopic approaches have failed or are not feasible [7].
Treatment in special clinical situations
Table 2 provides a summary of treatment options and key considerations across special clinical situations.
Table 2.
Treatment options for urolithiasis in special clinical situations.
| Situation | ESWL | RIRS (fURS) | PCNL | Key considerations | Grade |
|---|---|---|---|---|---|
| Horseshoe kidney | SFR 31–47%; impaired drainage limits fragment clearance [14] | SFR 60–100%; comparable overall SFR to PCNL; predominantly minor complications [14] | SFR 80–95%; technically demanding; highest complication burden [14] | RIRS may be favored for selected small-to-moderate stones when lower morbidity is prioritized; PCNL for large or complex burden [14] | B RIRS/PCNL |
| Pelvic ectopic kidney | SFR 38–66%; bony pelvic interposition limits stone targeting [13] | SFR 60–94%; ureteral tortuosity may limit instrument deflection [12] | SFR 75–88%; ultrasound- or laparoscopy-assisted access recommended [13] | Treatment should be individualized according to anatomy; referral to an expert center is advisable in all cases [13] | C all modalities |
| Solitary kidney | Risk of steinstrasse; post-ESWL obstruction may precipitate AKI [1] | Preferred modality; lowest parenchymal aggressiveness [1, 12] | Indicated for large stones; miniaturized techniques preferred [1] | Strict perioperative renal function monitoring is mandatory; any complication may precipitate AKI requiring RRT [1, 3] | C fURS preferred |
| Pregnancy | Absolutely contraindicated throughout pregnancy [1, 3] | SFR 80–90%; safe in experienced hands; 2nd trimester preferred [15] | Reserved for exceptional cases only [15] | Double-J stent or PCN for initial decompression; minimize fluoroscopy; post-URS stent recommended [15] | B URS; C decompression |
| Pediatric patients | First-line for ureteral stones < 10 mm and renal stones < 20 mm (EAU) [1, 16] | Safe and effective in experienced centers; SFR > 96% for ureteral stones [16] | Mini- or ultra-mini PCNL for stones > 20 mm; improved complication profile vs. standard PCNL [16] | ALARA principle for imaging; stone analysis and metabolic evaluation mandatory in all cases [1, 3, 16] | A ESWL/PCNL |
Notes: ESWL: extracorporeal shock wave lithotripsy; AKI: acute kidney injury; ALARA: as low as reasonably achievable; fURS: flexible ureterorenoscopy; PCN: percutaneous nephrostomy; PCNL: percutaneous nephrolithotomy; RIRS: retrograde intrarenal surgery; RRT: renal replacement therapy; SFR: stone-free rate; URS: ureteroscopy.
HK
HK is the most common congenital renal anomaly, with a reported incidence of 1/400–1/666 [14]. Fusion of the lower poles generates an isthmus of functional parenchyma preventing normal embryological ascent and rotation, resulting in malrotation, anterior displacement of the collecting system, and variable ureteropelvic junction obstruction. These changes, together with associated metabolic abnormalities, increase the risk of
stone formation in up to 60% of patients with HK [14].
ESWL yields suboptimal results in HK due to impaired fragment clearance and difficult stone targeting [14]. RIRS
is increasingly adopted in HK, though the anomalous anatomy, including flattened pelves, narrow intrarenal spaces, and the length of the instrument remaining outside the urethra, reduces maneuverability and may lower single-session SFRs [12, 14]. A 2023 systematic review and meta-analysis (9 retrospective studies; 565 patients) found no statistically significant difference in overall SFR between PCNL and RIRS in HK (RR 1.04; 95% CI 0.95–1.13; I² = 20.63%), while RIRS was associated with fewer and less severe complications [14]. RIRS was significantly more effective than ESWL, with a higher overall SFR (RR 1.38; 95% CI 1.04–1.82; I² = 0%) [14]. PCNL achieves higher single-session SFRs for large stones but carries the highest complication burden in this population, including cases of CD grade III–IV events [14]. Based on available evidence, RIRS appears to be an attractive option for selected small-to-moderate stones in HK when lower morbidity is prioritized, whereas PCNL remains important for larger or more complex stone burdens [1, 13, 14].
Pelvic ectopic kidney
Pelvic ectopic kidney (PEK) results from failure of normal renal ascent during embryological development, with an incidence of approximately 1/2,000–1/3,000 [13]. Structural anomalies, including high ureteral insertion, malrotation, aberrant vascular supply, and proximity to pelvic organs, predispose to urinary stasis and stone formation. Treatment outcomes are consistently lower than in normally positioned kidneys across all modalities [12, 13]. PCNL with ultrasound- or laparoscopy-assisted access achieves the highest SFRs (75–88%) but demands significant expertise given the proximity to pelvic structures [13]. RIRS is limited by ureteral tortuosity, though modern smaller-caliber instruments have improved accessibility [12]. Treatment should be individualized and referral to a center of expertise is advisable in all cases [13].
Solitary kidney
Patients with a solitary kidney, whether congenital, post-nephrectomy, or functionally excluded, represent a high-risk clinical scenario in which any procedure-related complication threatening renal function may precipitate acute kidney injury (AKI) requiring renal replacement therapy. fURS is the preferred modality owing to its low parenchymal aggressiveness and absence of percutaneous access [1, 12] (Oxford Level 4; Grade C). ESWL may be considered for small stones with favorable anatomy but carries the risk of post-ESWL steinstrasse, which constitutes a urological emergency in the solitary kidney requiring immediate decompression [1]. PCNL is indicated for large stones or when retrograde approaches have failed, using miniaturized techniques where possible [1, 3]. Strict perioperative renal function assessment and close postoperative monitoring are mandatory in this population [1, 3].
Pregnancy
Symptomatic ureteral stones during pregnancy require a management strategy that simultaneously addresses maternal stone disease and minimizes risk to the fetus. When conservative management, hydration, analgesia and urine straining, fails to achieve stone passage, or complications arise (infection, refractory obstruction, renal deterioration), active intervention is indicated [15]. Temporary decompression with a double-J stent or percutaneous nephrostomy is the safest initial approach, particularly in the first trimester, as it avoids the need for general anesthesia [15] (Oxford Level 4; Grade C). Definitive ureteroscopy with holmium laser lithotripsy is a feasible option in experienced hands, preferably performed during the second trimester with minimal fluoroscopic exposure and ultrasound guidance where possible [15]. A recent systematic review confirmed SFRs of 80–90% with low maternal complication rates (hematuria, urinary tract infection, transient uterine contractions) and no relevant adverse fetal outcomes when performed by experienced operators [15] (Oxford Level 2a; Grade B). Postoperative double-J stent placement is recommended following ureteroscopy in pregnancy [15]. ESWL is absolutely contraindicated throughout pregnancy [1, 3] (Oxford Level 5; Grade D).
Pediatric patients
Pediatric urolithiasis has increased in incidence in recent decades, with a variable and frequently non-specific clinical presentation [16]. The as low as reasonably achievable (ALARA) principle must guide diagnostic imaging, with ultrasound as the primary modality [1]. Treatment indications broadly parallel those in adults: ESWL is the EAU-recommended first-line option for ureteral stones < 10 mm and renal stones < 20 mm; mini- or ultra-mini PCNL is the treatment of choice for stones > 20 mm, offering high SFRs with an improved complication profile compared with standard PCNL in pediatric patients [1, 3, 16]. Ureteroscopy with laser lithotripsy is safe and effective in experienced pediatric stone centers [16]. Stone composition analysis and metabolic evaluation are mandatory in all pediatric patients to guide preventive strategies [1, 3, 16].
Surgical treatment of ureteral stones
Table 3.
Recommended treatment options for ureteral stones by location and size.
| Location | Size | First-line (EAU) | First-line (AUA) | Key supporting evidence | Grade |
|---|---|---|---|---|---|
| Proximal ureter | < 10 mm | ESWL or URS | ESWL or URS | Comparable SFR between modalities; URS associated with faster stone-free status [1, 3] | A |
| Proximal ureter | > 10 mm | URS (1st line); ESWL (2nd line) | ESWL or URS (equivalent) | Antegrade URS yields higher SFR than retrograde approach (SFRR 1.14; 95% CI 1.10–1.19) [15]. LU achieves higher initial SFR than PCNL (OR 3.26; 95% CI 1.45–7.31; P = 0.004) [7]. For large stones, PCNL and LU achieve higher SFR than URS alone [17] | A |
| Distal ureter | < 10 mm | ESWL or URS | URS (1st line); ESWL (2nd line) | MET with alpha-blockers increases spontaneous expulsion [2, 3]. Emergency ESWL superior to delayed ESWL (RR 1.22; 95% CI 1.13–1.32; no increase in complications) [18] | A |
| Distal ureter | > 10 mm | URS (1st line); ESWL (2nd line) | URS (1st line); ESWL (2nd line) | URS achieves SFR > 90% for distal ureteral stones [1, 3]. Routine post-URS stenting may be safely omitted after uncomplicated URS [1, 3] | A |
Notes: AUA, American Urological Association; EAU, European Association of Urology; ESWL: extracorporeal shock wave lithotripsy; LU: laparoscopic ureterolithotomy; MET: medical expulsive therapy; PCNL: percutaneous nephrolithotomy; SFRR: stone-free rate ratio; SFR: stone-free rate; URS: ureteroscopy.
Proximal ureteral stones
Proximal ureteral stones (PUS), defined as those located above the iliac vessels, carry a greater risk of endoscopic retropulsion into the renal pelvis during manipulation than distal stones. For PUS < 10 mm, both ESWL and ureteroscopy (URS) are acceptable first-line options [1, 3]. For PUS > 10 mm, the EAU recommends URS as first-line treatment and ESWL as second-line; the AUA considers both modalities equivalent in this size range [1, 3]. A systematic review and meta-analysis comparing antegrade versus retrograde ureteroscopic lithotripsy for PUS > 10 mm demonstrated a significantly higher SFR with the antegrade approach (stone-free rate ratio [SFRR] 1.14; 95% CI 1.10–1.19), with a shorter hospital stay favoring the retrograde approach [19]. For stones in which both ESWL and retrograde URS have failed, laparoscopic ureterolithotomy achieves higher initial SFRs than PCNL (OR 3.26; P = 0.004) with a lower transfusion rate, though operative time is significantly longer [7]. Meta-analytic data from 12 RCTs confirm that PCNL and LU achieve higher SFRs than URS alone for large proximal ureteral stones, with URS associated with a higher ureteral injury rate in this setting [17].
Distal ureteral stones
Distal ureteral stones carry a substantially higher spontaneous expulsion rate than proximal stones, particularly for small calculi. Medical expulsive therapy (MET) with alpha-1 adrenergic blockers (tamsulosin 0.4 mg/day) is recommended by both EAU and AUA guidelines for stones ≤ 10 mm without complications, as contextual background to the decision for active surgical treatment [1, 3]. When active intervention is indicated, URS with laser lithotripsy is the preferred option given its consistently high SFR, particularly for stones > 10 mm [1, 3]. A meta-analysis of 9 studies encompassing 976 patients demonstrated that emergency ESWL achieves a significantly higher 4-week SFR than delayed ESWL (RR 1.22; 95% CI 1.13–1.32) without increasing complication rates [18], supporting early intervention when ESWL is the selected modality. Routine pre-URS double-J stenting is not recommended for uncomplicated ureteral stones, as it does not improve SFR and adds stent-related morbidity [1, 3]. Post-URS stenting may similarly be omitted following uncomplicated procedures without increasing postoperative adverse events [1, 3]. An integrated treatment algorithm is provided in Figure 1.
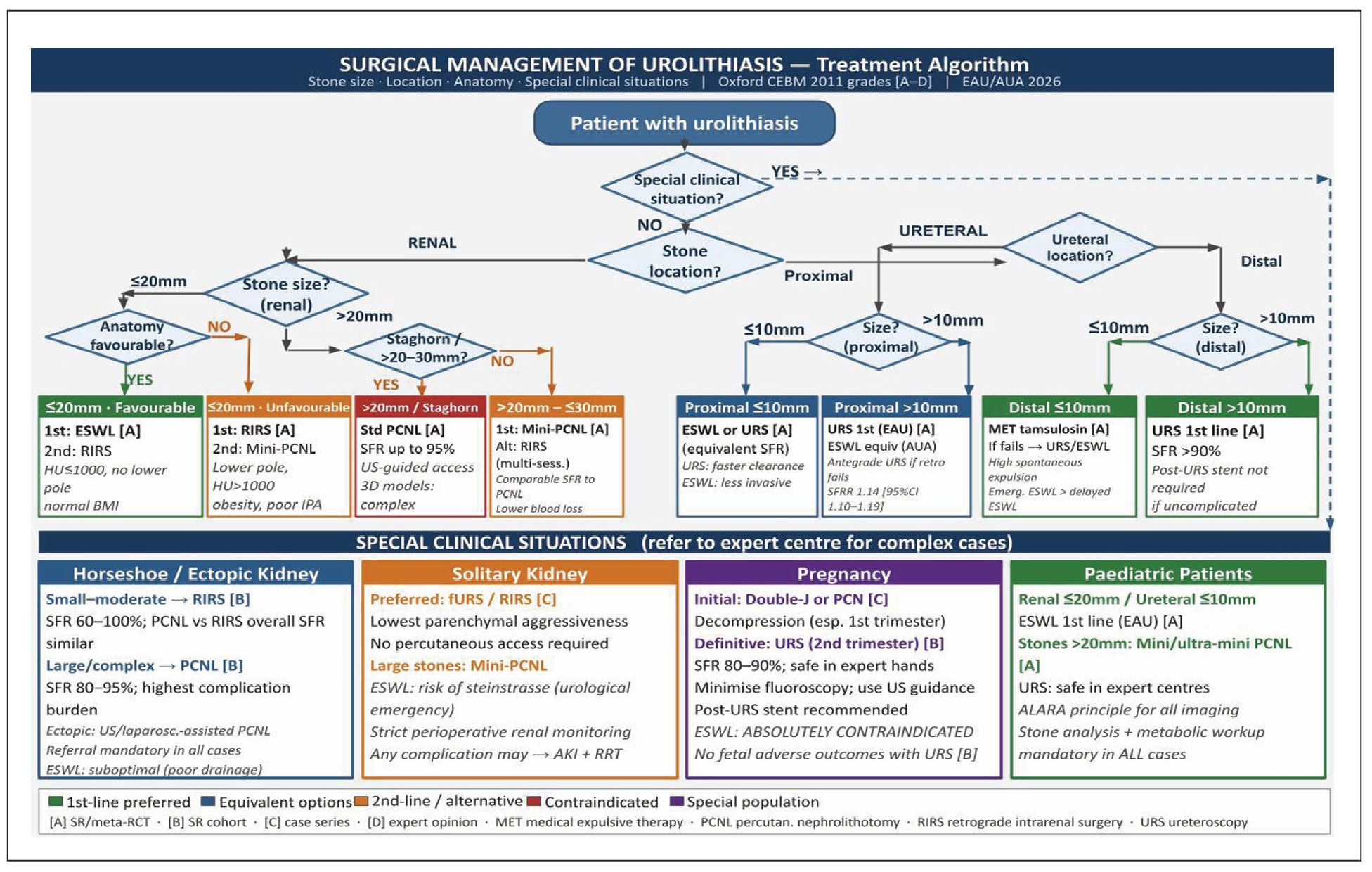
Figure 1. Treatment algorithm for the surgical management of urolithiasis according to stone size, location, patient anatomy, and special clinical situations. Recommendation grades follow the Oxford Centre for Evidence-Based Medicine (Oxford CEBM) 2011 Levels of Evidence. Abbreviation: ESWL, extracorporeal shock wave lithotripsy; fURS, flexible ureterorenoscopy; IPA, infundibulopelvic angle; MET, medical expulsive therapy; PCN, percutaneous nephrostomy; PCNL, percutaneous nephrolithotomy; RIRS, retrograde intrarenal surgery; SFR, stone-free rate; URS, ureteroscopy.
Conclusions
The key evidence base underpinning the conclusions of this review is summarized in Table 4. The surgical management of urolithiasis is characterized by an evolving and largely effective array of minimally invasive options whose optimal application depends critically on individualization rather than modality preference. ESWL remains a valid, guideline-endorsed first-line option for appropriately selected patients and should not be marginalized in contemporary practice. RIRS is increasingly used for small-to-moderate renal stones across a wide range of clinical scenarios, driven by genuine advances in flexible ureteroscope technology and laser lithotripsy; however, treatment selection must continue to be guided by stone burden, collecting system anatomy, patient comorbidities, and local surgical expertise [1, 3, 8, 9]. PCNL, including its miniaturized variants, remains the most effective single-session treatment for large and complex stones, and continues to evolve in terms of access technique and instrument design. In anatomically complex situations and special clinical populations, decisions require particularly careful individualization and, in many cases, referral to centers with dedicated endourological expertise [13, 14]. Newer laser platforms, particularly the TFL and p-Tm:YAG, show promising technical advantages, but their definitive superiority over contemporary Ho:YAG systems across the full range of clinical scenarios remains to be established [4, 5]. The field would benefit substantially from well-designed randomized controlled trials with standardized outcome reporting, particularly for intermediate-size renal stones, anatomically complex presentations, and pediatric populations.
Table 4.
Selected key evidence informing current surgical management of urolithiasis.
| Topic | Reference | Study design | N | Comparison / focus | Key findings | Clinical implication |
|---|---|---|---|---|---|---|
| Clinical practice guidelines | [1, 3] | Clinical practice guidelines | — | EAU and AUA recommendations on surgical management of renal and ureteral stones | Both guidelines recommend ESWL, RIRS, and PCNL as standard options; indications vary by stone size, location, and patient factors. Minor divergences exist for proximal ureteral stones and pediatric patients. | Provides the authoritative framework for treatment selection; guideline concordance supports individualization based on stone burden, anatomy, and local expertise |
| Renal stones | Ying et al. [9] | Systematic review and meta-analysis | NR | RIRS vs. PCNL for renal stones | Comparable SFR for stones ≤ 20 mm; PCNL superior for stones > 20 mm, with higher morbidity. | Supports the expanding role of RIRS for selected small-to-moderate renal stones, while PCNL remains the preferred option for larger stone burdens |
| Renal stones/fURS | He et al. [8] | Narrative review | — | Advances in fURS for renal stones | Single-use ureteroscopes and newer laser platforms may broaden the indications for RIRS; reduced repair costs and comparable performance to reusable devices. | Supports the growing role of RIRS in contemporary stone surgery; indications should remain individualized according to anatomy, stone burden, and local expertise |
| URS: expanding roles | Ho et al. [10] | Narrative review | — | Expanding indications for URS in complex stone disease and special populations | URS demonstrated good outcomes across large stones, bilateral disease, obesity, pregnancy, pediatric patients, solitary kidney, and horseshoe kidney. | Establishes URS as a versatile option beyond standard indications; underpins the rationale for evaluating RIRS in anatomically and clinically complex scenarios |
| Complications across modalities | Grosso et al. [6] | Systematic review | > 14,000 | Complications of RIRS, PCNL, and URS | Major complications (CD ≥ III) were uncommon after RIRS and more frequent after PCNL; urosepsis ranged from 1% to 6.6% across modalities. | Highlights the higher morbidity profile of PCNL relative to retrograde endoscopic approaches; supports preference for RIRS when morbidity minimization is a priority |
| Anatomical selection for RIRS | Geavlete et al. [12] | Narrative review | — | Unfavorable anatomical factors for fURS | Acute infundibulopelvic angle, long infundibular length, and congenital renal anomalies (horseshoe kidney, ectopic kidney) may reduce RIRS efficacy and increase instrument damage risk. | Reinforces the importance of preoperative pelvicalyceal anatomy assessment when selecting candidates for RIRS; identifies scenarios where alternative approaches should be considered |
| Proximal ureteral stones | Taguchi et al. [19] | Systematic review and meta-analysis | NR | Antegrade vs. retrograde ureteroscopic lithotripsy for proximal ureteral stones > 10 mm | Antegrade approach achieved higher SFR (SFRR 1.14; 95% CI 1.10–1.19); retrograde approach associated with shorter hospital stay. | Suggests antegrade URS may offer superior clearance for selected large proximal ureteral stones, at the cost of greater invasiveness; retrograde remains appropriate for most patients |
| Large proximal ureteral stones | Chang et al. [7] | Systematic review and meta-analysis | 933 | LU vs. PCNL | LU achieved higher initial SFR (OR 3.26; 95% CI 1.45–7.31; P = 0.004) and lower transfusion rate (OR 0.13; P = 0.007), but longer operative time; final SFR was comparable between groups. | Supports LU as an effective alternative for selected large proximal ureteral stones when endoscopic approaches are unsuitable or unsuccessful; not recommended as routine first-line option |
| Large proximal ureteral stones | Lai et al. [17] | Systematic review and meta-analysis of randomized trials | 1416 | URS vs. PCNL vs. LU for proximal ureteral stones > 10 mm | URS showed lower SFR than PCNL and LU (both P < 0.05); ureteral injury was more frequent with URS (RR 4.11–5.27 vs. PCNL and LU); no significant difference between PCNL and LU in SFR or overall complications. | Suggests PCNL and LU provide greater stone clearance than URS for large proximal ureteral stones; choice between PCNL and LU should be guided by local expertise and patient factors |
| Ureteral stones / ESWL timing | Peng et al. [18] | Meta-analysis | 976 | Emergency vs. delayed ESWL for ureteral stones | Emergency ESWL improved 4-week SFR (RR 1.22; 95% CI 1.13–1.32), shortened stone-free time, and reduced need for auxiliary procedures; complication rates were not significantly different between groups | Supports early ESWL as a clinically reasonable strategy in patients with acute ureteral stones when ESWL is the selected modality; reduces stone burden duration and secondary intervention rates |
| Horseshoe kidney | Qaoud et al. [14] | Systematic review and meta-analysis | 565 | PCNL vs. RIRS vs. ESWL in horseshoe kidney | No significant difference in overall SFR between PCNL and RIRS (RR 1.04; 95% CI 0.95–1.13; I² = 20.63%); RIRS outperformed ESWL (RR 1.38; 95% CI 1.04–1.82; I² = 0%); RIRS showed a more favorable complication profile | Supports RIRS as an attractive option for selected small-to-moderate stones in horseshoe kidney when lower morbidity is prioritized; PCNL remains important for larger or more complex stone burdens |
| Pelvic ectopic kidney | Salvi et al. [13] | Systematic review | NR | Active treatment of renal stones in pelvic ectopic kidney | Reported SFRs: ESWL 38–66%, RIRS 60–94%, PCNL 75–88%; all modalities technically more demanding than in normally positioned kidneys | Indicates treatment should be individualized according to collecting system anatomy; ultrasound- or laparoscopy-assisted PCNL should be reserved for experienced centers; referral advisable |
| Pregnancy | Laranjo-Tinoco et al. [15] | Systematic review | NR | URS for ureteral stones during pregnancy | URS achieved of 80–90%, with predominantly minor maternal complications (hematuria, UTI, transient uterine contractions) and no relevant adverse fetal outcomes reported | Supports ureteroscopic laser lithotripsy as a safe and effective option during pregnancy in experienced hands; ESWL is absolutely contraindicated; double-J stent placement postURS is recommended |
| Laser technology | Yu et al. [4] | Narrative review | — | Ho:YAG, Moses technology, and TFL in fURS | TFL showed higher water absorption (4–5 × vs. Ho:YAG), compatibility with smaller fibres (50–150 µm), and reduced retropulsion in experimental and early clinical studies; Moses 2.0 operates up to 120 Hz | Suggests TFL offers promising technical advantages over conventional Ho:YAG; definitive clinical superiority across all scenarios remains unconfirmed and requires larger prospective comparative trials |
| Laser technology | Hernandez-Gaytan et al. [5] | Mini-review | — | p-Tm:YAG laser for lithotripsy | Early series reported effective ablation, minimal retropulsion, fine dust production, and high SFR with low morbidity; evidence derives from small single-center experiences | Suggests p-Tm:YAG is a promising emerging platform occupying a middle ground between Ho:YAG and TFL; larger prospective studies are needed before routine clinical recommendations can be made |
| Guideline comparison | Akram et al. [11] | Comparative guideline review | — | EAU vs. AUA guidance on renal and ureteral stone management | Broad agreement between EAU and AUA guidelines; minor divergences in proximal ureteral stones > 10 mm and pediatric lithiasis; both guidelines advocate individualized, evidence-based decision-making | Helps contextualize current practice recommendations and identifies areas of ongoing controversy between major guidelines; supports the need for further RCTs to resolve current uncertainties |
Notes: AUA, American Urological Association; CD, Clavien-Dindo; CI, confidence interval; EAU, European Association of Urology; ESWL, extracorporeal shock wave lithotripsy; fURS, flexible ureterorenoscopy; Ho:YAG, holmium:yttrium-aluminium-garnet; LU, laparoscopic ureterolithotomy; NR, not reported; OR, odds ratio; PCNL, percutaneous nephrolithotomy; p-Tm:YAG, pulsed thulium:yttrium-aluminium-garnet; RCT, randomized controlled trial; RIRS, retrograde intrarenal surgery; RR, risk ratio; SFR, stone-free rate; SFRR, stone-free rate ratio; TFL, thulium fiber laser; URS, ureteroscopy; UTI, urinary tract infection. Representative studies were selected according to their clinical relevance, methodological quality, and contribution to the main topics covered in this narrative review. Studies are presented in thematic order rather than in order of citation in the manuscript.
Declarations
Acknowledgments
The authors wish to acknowledge the clinical teams and researchers whose work in the field of urolithiasis and endourology has made this review possible. The authors also thank the investigators whose sustained efforts have generated high-level evidence in the surgical management of urinary stone disease.
Author contributions
Miguel Ángel Arrabal Polo: conceptualization, literature search, methodology, supervision, and project administration. Alberto Zambudio Munuera: conceptualization, literature search, methodology, data collection, writing original draft, writing review and editing, and project administration. Miguel Arrabal Martín: review and editing, supervision, and project administration. Irene Millán Ramos: data collection and writing review and editing. Patricia Rodríguez Parras: data collection and writing review and editing. Ana Morales Martinez: writing, review and editing. María Teresa Melgarejo Segura: writing, review and editing. Francisco Gutiérrez Tejero: writing, review and editing. All authors read and approved the final version of the manuscript.
Availability of data and materials
No new datasets were generated or analyzed during the preparation of this study. All data supporting the findings are available within the cited publications.
Financial support and Sponsorship
None.
Conflicts of Interest
All authors declared that there are no conflicts of interest.
Ethical approval and consent to participate
Not applicable.
Consent for publication
Not applicable.
References
1. Uroweb. Arnhem, The Netherlands: European Association of Urology, c2026 [cited 2026 May 12]. Available from: https://uroweb.org/guidelines/urolithiasis.
2. Raheem O, Khandwala Y, Sur R, Ghani K, & Denstedt J. Burden of urolithiasis: trends in prevalence, treatments, and costs. Eur Urol Focus, 2017, 3(1): 18-26. [Crossref]
3. AUA. Linthicum, MD: American Urological Association; c2026 [cited 2026 May 12]. Available from: https://www.auanet.org/guidelines-and-quality/guidelines/surgical-management-of-kidney-and-ureteral-stones.
4. Yu S, Liu L, Li Y, Zhou L, Chen J, Li H, et al. Flexible ureteroscopic treatment of kidney stones: how do the new laser systems change our concepts? Asian J Urol, 2024, 11(2): 156-168. [Crossref]
5. Hernandez-Gaytan C, Proietti S, Leonardis F, Mongelli L, Gaboardi F, & Giusti G. Pulsed thulium:YAG laser for lithotripsy. Eur Urol Focus, 2025, 11(5): 725-729. [Crossref]
6. Grosso A, Sessa F, Campi R, Viola L, Polverino P, Crisci A, et al. Intraoperative and postoperative surgical complications after ureteroscopy, retrograde intrarenal surgery, and percutaneous nephrolithotomy: a systematic review. Minerva Urol Nephrol, 2021, 73(3): 309-332. [Crossref]
7. Chang X, Yang Z, Wang X, Wang H, Wang Y, & Han Z. Laparoscopic ureterolithotomy versus percutaneous nephrolithotomy for large proximal ureteral stones: a systematic review and meta-analysis. Wideochir Inne Tech Maloinwazyjne, 2023, 18(1): 42-51. [Crossref]
8. He M, Dong Y, Cai W, Cai J, Xie Y, Yu M, et al. Recent advances in the treatment of renal stones using flexible ureteroscopys. Int J Surg, 2024, 110(7): 4320-4328. [Crossref]
9. Ying Z, Ming S, Yang R, Zou B, Jia Y, Shu M, et al. Comparison of safety and efficacy of negative pressure aspiration assisted retrograde intrarenal surgery and traditional percutaneous nephrolithotomy in the treatment of upper urinary tract stones larger than 2 cm: a systematic review and meta-analysis. Int J Surg, 2025, 111(5): 3613-3628. [Crossref]
10. Ho A, Sarmah P, Bres-Niewada E, & Somani B. Ureteroscopy for stone disease: expanding roles in the modern era. Cent European J Urol, 2017, 70(2): 175-178. [Crossref]
11. Cui D, Yan F, Yi J, He D, Zhang Y, Zhang Z, et al. Efficacy and safety of 3D printing-assisted percutaneous nephrolithotomy in complex renal calculi. Sci Rep, 2022, 12(1): 417-429. [Crossref]
12. Geavlete B, Mareș C, Popescu R, Mulțescu R, Ene C, & Geavlete P. Unfavorable factors in accessing the pelvicalyceal system during retrograde flexible ureteroscopy (fURS). J Med Life, 2023, 16(3): 372-380. [Crossref]
13. Salvi M, Muto G, Tuccio A, Grosso AA, Mari A, Crisci A, et al. Active treatment of renal stones in pelvic ectopic kidney: systematic review of literature. Minerva Urol Nefrol, 2020, 72: 691-697. [Crossref]
14. Qaoud Y, Al Tali M, Boland F, Simpson A, & Davis N. Comparative evaluation of urolithiasis management options in patients with horseshoe kidney: a systematic review and meta-analysis. Curr Urol, 2023, 17(3): 193-205. [Crossref]
15. Laranjo Tinoco C, Oliveira M, Araújo A, Cardoso A, Oliveira C, Mota P, et al. Surgical management of obstructing ureteral stones during pregnancy: a systematic review of different techniques. Arch Ital Urol Androl, 2024, 96(3): 12153. [Crossref]
16. Sultan S, Aba Umer S, Ahmed B, Naqvi SAA, & Rizvi SAH. Update on surgical management of pediatric urolithiasis. Front Pediatr, 7:252. [Crossref]
17. Lai S, Jiao B, Diao T, Seery S, Hu M, Wang M, et al. Optimal management of large proximal ureteral stones (> 10 mm): a systematic review and meta-analysis of 12 randomized controlled trials. Int J Surg, 2020, 80: 205-217. [Crossref]
18. Peng C, Lou Y, Xu L, Wu G, Zhou X, Wang K, et al. Efficacy of emergency extracorporeal shock wave lithotripsy in the treatment of ureteral stones: a meta-analysis. BMC Urol, 2023, 23(1): 56-68. [Crossref]
19. Taguchi K, Hamamoto S, Osaga S, Sugino T, Unno R, Ando R, et al. Comparison of antegrade and retrograde ureterolithotripsy for proximal ureteral stones: a systematic review and meta-analysis. Transl Androl Urol, 2021, 10(3): 1179-1191. [Crossref]